
Oral / Halitosis Integrated Triage: Find the Source First, Then Choose the Specialty
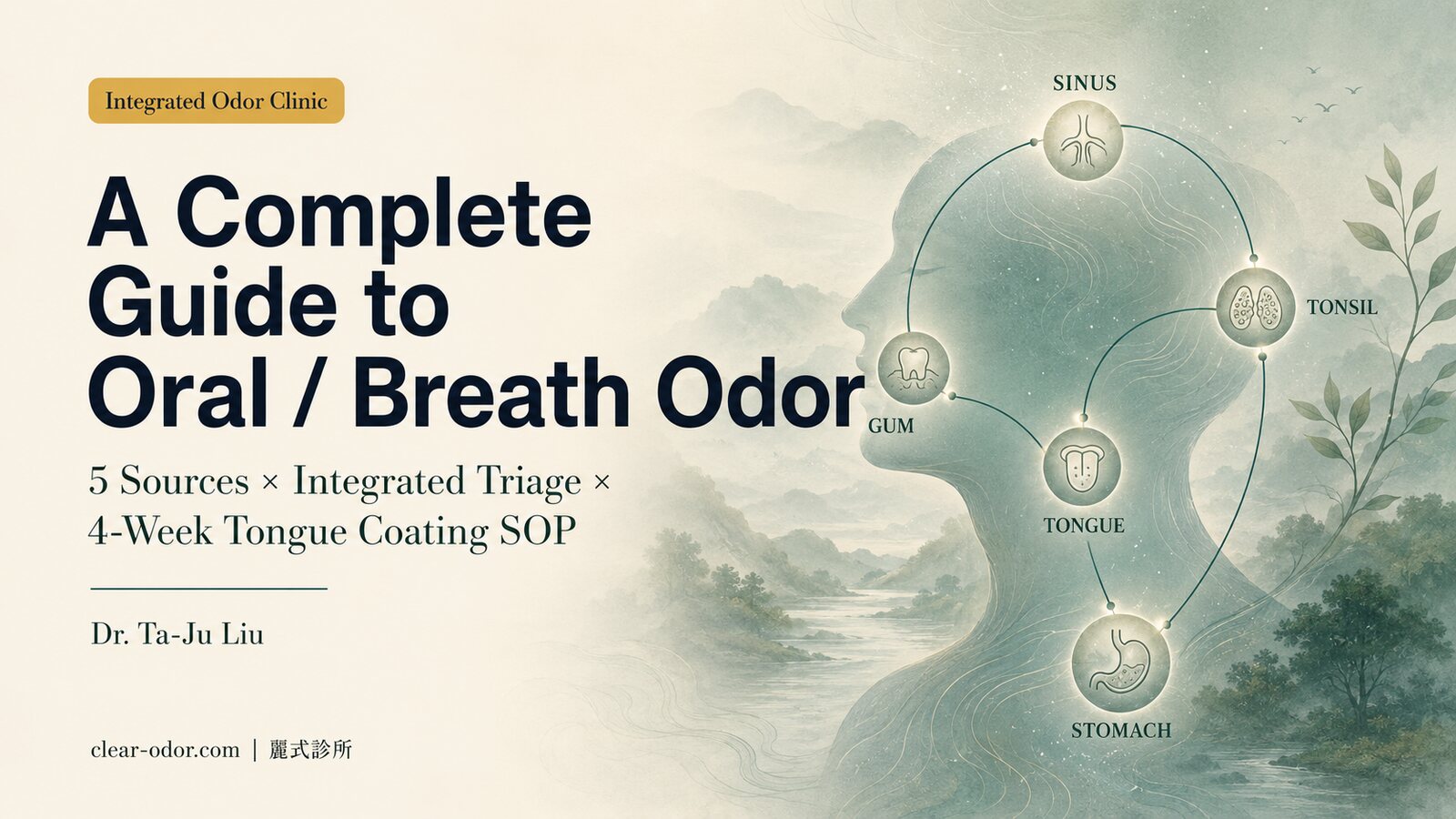
5-Source IdentificationIntegrated Framework for Dental / ENT / GI Referral
Halitosis is one of the most commonly mistreated odor sites — its sources are at least five (tongue coating / periodontal / tonsil stones / post-nasal drip / GERD), each requiring different specialty management, and they often coexist. The integrated odor clinic's role is not to treat everything itself, but to perform integrated triage first, identify the primary source, then deliver a personalized referral path — sparing you the cycle of switching doctors and repeating surface-level treatments.
Why does halitosis need "integrated triage"?
- Over 90% of halitosis originates in the oral cavity (tongue coating, periodontal, saliva). But "I feel I smell despite brushing" often signals the other 10% — multi-source or atypical origins.
- A single specialty (pure dental or pure ENT) tends to look only within its own domain — missing cross-specialty causes (e.g., periodontal + post-nasal drip co-existing).
- A subset falls into the OlRS gray zone (strong self-perception, normal objective findings) — they need a different management path, not yet another cleaning.
- The integrated clinic's value is identification and routing — getting you to the specialty that can actually solve it, avoiding time wasted on wrong paths.
Halitosis: 5 Sources × Triage Path
During the initial consultation, we evaluate each of these 5 sources and identify your primary and secondary sources (most people have primary + 1-2 secondary). We then decide which station to address first and which specialty leads.
Tongue Coating (VSCs)
→ This Clinic + DentalMechanism
Anaerobic bacteria on the posterior 1/3 of the dorsum break down food debris and shed epithelium, producing volatile sulfur compounds (H₂S, methyl mercaptan) — the classic "rotten" smell.
Initial Action
Tongue coating index assessment + tongue brush education + 4-week home protocol; if <50% improvement at 4 weeks, refer to dental.
Periodontal Disease / Caries
→ Dental (Periodontics-first)Mechanism
Anaerobic bacteria in periodontal pockets, deep caries, and faulty restorations form biofilms — chronic inflammation + protein degradation produce odor.
Initial Action
Initial gingival bleeding index + oral hygiene assessment; immediate referral to trusted periodontics for professional cleaning and deeper management.
Tonsilloliths (Tonsil Stones)
→ ENTMechanism
Calcified food debris and shed epithelium accumulated in tonsillar crypts contain high sulfur concentrations — characteristic "putrid" smell.
Initial Action
Clinical inspection of tonsillar crypts; if suspected, refer to ENT for extraction, laser cryptolysis, or tonsillectomy evaluation.
Post-Nasal Drip
→ ENTMechanism
Chronic sinusitis or allergic rhinitis causes mucus drainage; protein-rich secretions enter the oropharynx and are metabolized by bacteria.
Initial Action
Evaluate nasal congestion, drip symptoms, allergy history; if needed, refer to ENT for sinus CT or nasal endoscopy.
GERD (Reflux)
→ GI (Gastroenterology)Mechanism
Acidic gastric content (with partially digested protein) refluxes into the esophagus and oropharynx — accompanied by heartburn, belching, producing sour/acid odor.
Initial Action
Evaluate classic GERD symptoms; refer to GI for endoscopy or 24h pH monitoring as needed, paired with dietary modification.
* Most people have "primary source + 1-2 secondary sources" coexisting. Treat the primary first (4-8 weeks), reassess, then decide on secondary. We provide a triage report and referral letter you can hand to the specialist on visit.
When to See the Integrated Odor Clinic (Oral Triage)?
If any of the following apply, integrated triage first is preferable to directly booking a single specialty:
- You've seen dental + had cleanings + tried multiple mouthwashes, but halitosis persists
- You have multiple symptoms simultaneously (nasal congestion, drip, acid reflux) and aren't sure which specialty fits
- Family or colleagues mention odor, but you don't notice it yourself after brushing
- You perceive strong odor but others don't (OlRS gray-zone evaluation)
- Odor at multiple body sites (underarm, scalp, foot) needing integrated handling
Oral triage is performed during the in-person Odor Map initial consultation. Book on LINE; fee and duration are individualized based on your described condition.
Frequently Asked Questions
Q1.Will Clear Odor Clinic treat my halitosis directly?
Q2.Why not go directly to dental or ENT?
Q3.Can halitosis be "cured"?
Q4.I've had tonsil stones extracted but they keep coming back — what now?
Q5.Is this suitable for children / teens?
Q6.Strong self-perception, others don't notice — what do I do?
Dr. Ta-Ju Liu
Lead Physician, Clear Odor Integrated Odor Clinic
"The key to halitosis isn't 'how well you brush' — it's 'where you brush.' Integrated triage routes you to the specialty that can actually solve it. That's the clinic's core value."
Do integrated triage first, then decide the next step
Don't keep cycling through wrong specialties. Book the Odor Map initial consultation on LINE — start with oral triage.
Book Odor Map ConsultationCan't use LINE? Leave us your contact details
Replies within 1 hour during business hours — we only use this info to respond
Learn More About Oral Odor
Oral / Breath Odor — A Complete Guide: Dr. Ta-Ju Liu on the 5 Main Sources Behind 'Why Brushing Alone Doesn't Work,' the Integrated Triage Framework, and When to Refer to Periodontics / ENT / GI
Breath odor is one of the most commonly mistreated complaints at the Integrated Odor Clinic — because there are at least 5 possible sources (tongue coating, periodontal disease, tonsil stones, post-nasal drip, GERD), each requiring a different specialty, and they frequently coexist. Dr. Ta-Ju Liu walks through the mechanisms behind each of the 5 sources, a 4-week home tongue-coating management SOP, the Tier 1-3 medical intervention ladder, and how to approach the grey-zone of Olfactory Reference Syndrome (ORS / OlRS). He also explains why starting with an Integrated Triage often saves more time than booking a single specialty directly — a reading framework that helps you understand which subtype you most likely belong to, and where to start, before you ever sit down for a consultation.
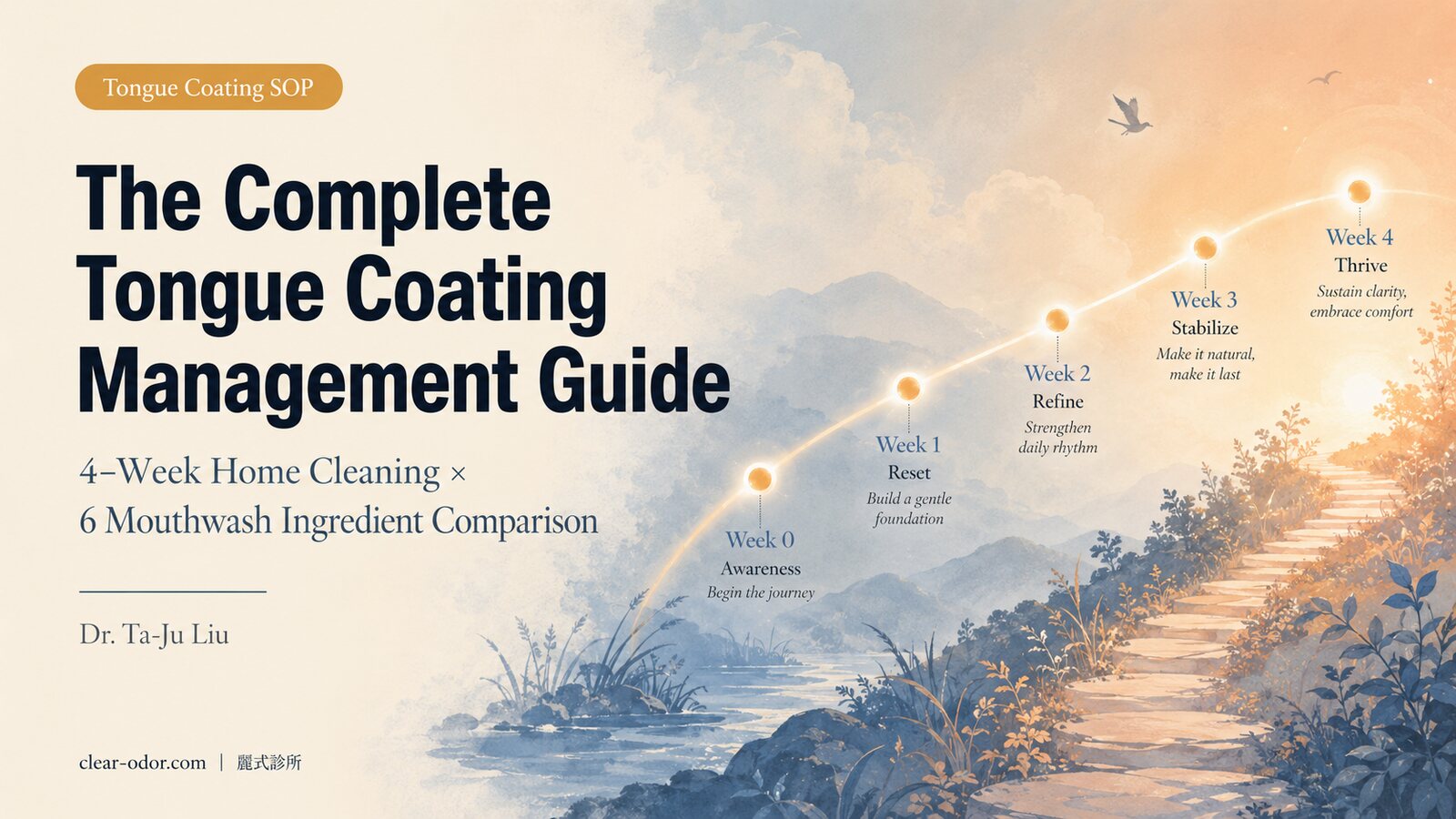
The Complete Tongue Coating Management Guide: Dr. Ta-Ju Liu on a 4-Week Home Cleaning Technique, Mouthwash Ingredient Comparison, and When to Step Up to Prescription Care
Tongue coating is the single largest source of oral malodor — accounting for 60-70% of cases. Yet most people get three things wrong when 'brushing the tongue': brushing the wrong area (only the tip, missing the posterior third), using the wrong tool (a regular toothbrush triggers the gag reflex), and choosing the wrong mouthwash (using chlorhexidine daily long-term alters the oral microbiome). This guide covers the dorsal tongue microecology and the chemistry of VSCs (volatile sulfur compounds), how to choose between a tongue scraper and a stainless-steel scraper, a comparison table of 6 mouthwash ingredients (chlorhexidine / essential oils / CPC / zinc / chlorophyll / oxygenating formulas), the week-by-week focus of a 4-week home SOP, and when to step up to prescription-grade chlorhexidine 0.12% or referral to Periodontics.
Multi-Source Coexistence in Halitosis: Dr. Ta-Ju Liu on Triage Sequencing and Cross-Specialty Integration for Periodontal + Sinus + GERD Comorbidity
Roughly 30-40% of chronic halitosis patients have a primary source coexisting with one or two secondary sources — tongue coating + periodontal disease, tongue coating + post-nasal drip, tonsilloliths + periodontal disease, and GERD + tongue coating are the four most common patterns. Looping back through a single specialty repeatedly tends to miss the real driver for 6 to 12 months. This guide walks through the identification cues for the five major sources, the handling sequence for the four typical comorbidity patterns, the timeline of cross-specialty referrals (periodontics → ENT → GI averages 4 to 8 weeks), how to choose between Integrated Triage and a direct single-specialty visit, and why 'identify the primary source first, then work through secondary sources in order' is more efficient than 'opening fire on all five fronts at once.'

Treatment Decision Framework for Sweat & Odor: Dr. Ta-Ju Liu on the 5-Dimension Decision Matrix, 4 Patient Scenarios, and the 'Minimum Viable Treatment' Principle
Facing the full spectrum of bromhidrosis, hyperhidrosis, and post-ETS compensatory sweating options, what most often paralyzes patients isn't 'which one is best,' but 'which one is best for me.' Dr. Ta-Ju Liu organizes a 5-dimension decision matrix (severity, timeline, budget, surgical tolerance, comorbidity), walks through 4 archetypal patient scenarios (17-year-old bullied teen / 32-year-old bride / 45-year-old man with combined odor + sweat / 22-year-old post-ETS), applies the 'Minimum Viable Treatment' principle, explains when to revisit the decision, and offers a consultation prep checklist. Designed to help you bring the right questions into the consultation room.
By age / cause axis
Only started after midlife — and will not wash off?
Aging odor × halitosis × systemic-metabolic — sort the source and the right specialist in the Midlife & Aging Odor guide
⚕️ Medical Disclaimer
The medical information provided on this page is for reference only and cannot replace individual face-to-face diagnosis, advice, or treatment from a physician. All medical procedures carry risks. Individual constitution and post-operative recovery vary from person to person. Please discuss any treatment plan with your attending physician before making decisions.