

Why Compare Rotational Curettage and Laser Side by Side
A common consultation question: "Doctor, with so many bromhidrosis surgery options out there, is rotational curettage better, or is laser?" There is no single answer — the two procedures use different mechanisms and suit different situations. Understanding the differences is what lets you make a decision that fits you. This article gives a fact-based comparison across 6 technical dimensions, not to make the choice for you, but to make the trade-offs visible.
A Single Table First — 6 Dimensions
| Dimension | Rotational Curettage | Laser |
|---|---|---|
| Mechanism | Mechanical removal under direct vision | Thermal destruction, partly blind |
| Incision size | About 4mm | About 3–5mm |
| Apocrine clearance rate | Complete clearance as the goal (under direct vision) | Limited by thermal penetration depth; literature varies |
| Recurrence rate | No recurrence reported in clinic 15-year follow-up | Higher in literature (tied to completeness of clearance) |
| Recovery | Same-day outpatient + 7-day pressure dressing | Same-day outpatient + 7-day pressure dressing |
| Cost | Usually higher (high manual-technique dependency) | More standardized, generally lower |
Below we expand on each dimension and the reasoning behind the choice.
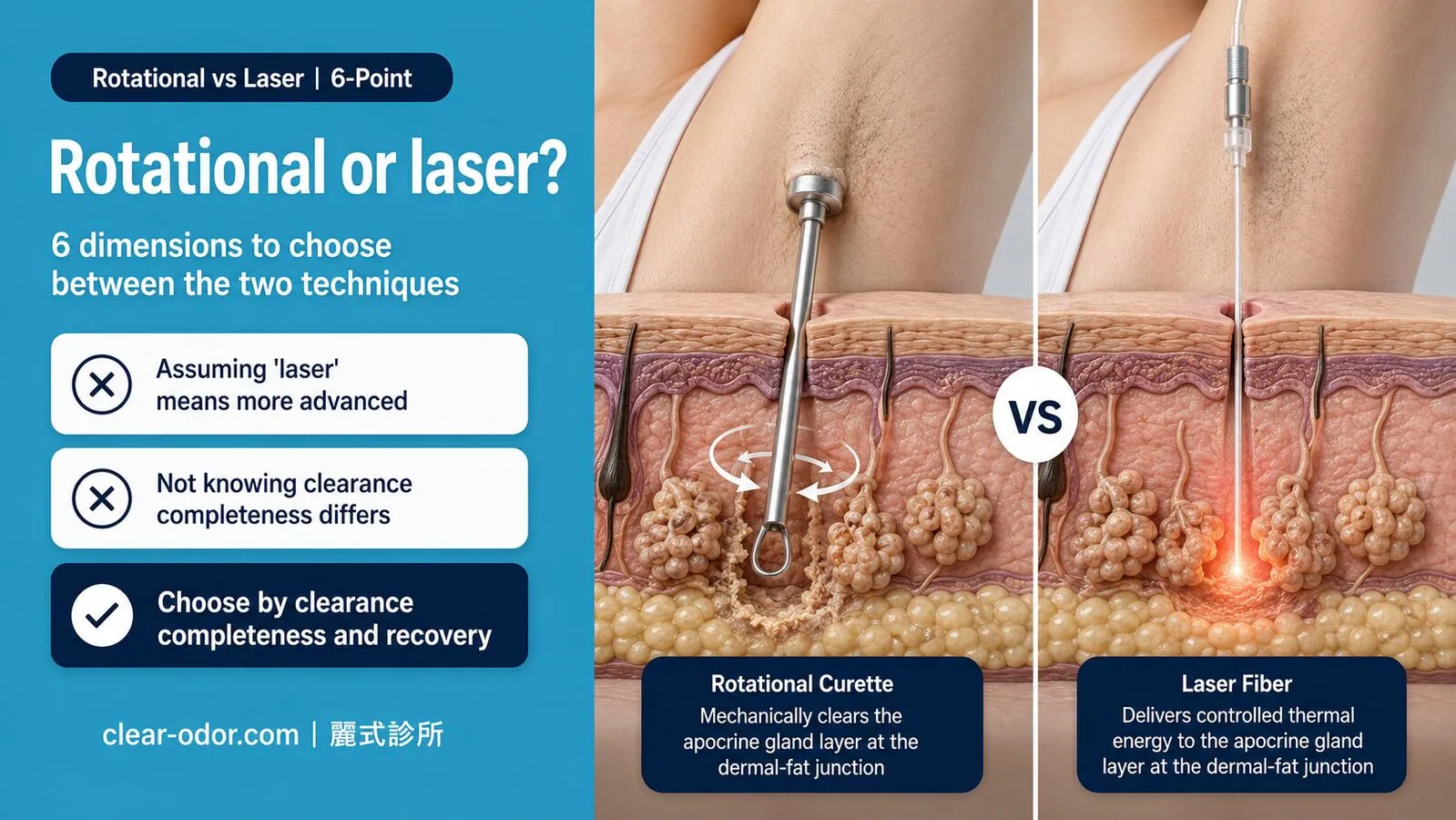
Dimension 1: Mechanism — Direct Vision vs Thermal Energy
Rotational curettage is built on "mechanical removal under direct vision." Through a 4mm incision and a lifted skin flap, the surgeon can directly see the dermal–subcutaneous interface where apocrine glands sit, then curette region by region. The whole process is eyes-on, hands-controlled — clearance progress can be judged in real time. Laser is built on "thermal destruction." A laser fiber enters through a small incision and emits heat to disrupt apocrine gland structures. The advantages are smaller-feeling incisions and a more standardized workflow; the trade-off is that thermal spread and depth depend on operator judgment, and portions of the procedure are blind — the surgeon cannot directly see exactly which layer the energy is reaching.Neither mechanism is "wrong" per se. The difference is whether clearance is verified under direct vision. For patients prioritizing thoroughness, the direct-vision mechanism offers higher controllability.
Dimension 2: Incision Size — Smaller Gap Than People Think
Rotational curettage uses about a 4mm incision; laser about 3–5mm — the size difference is not actually significant. Many patients assume "laser uses a smaller incision," but the numbers are close.
The real difference is not in incision size but in incision purpose:
- The rotational curettage incision is designed to lift the skin flap and create a direct-vision working space.
- The laser incision is designed for fiber entry; "opening to look" is not part of the design.
Cosmetically, scar conditions are similar; color and tension fade gradually over 3–6 months post-op. Final scar appearance is influenced more by individual skin biology than by procedure type, so it shouldn't be the deciding factor.
Dimension 3: Apocrine Clearance Rate — Visual Control vs Thermal Limits
This is where the two procedures differ most clearly.
Rotational curettage, because it's done under direct vision, lets the surgeon confirm in real time whether residual gland tissue remains. Complete apocrine gland clearance is the documented goal (per clinic records; individual results may vary). For patients prioritizing thorough clearance, this is the core advantage of the direct-vision mechanism. Laser, because it relies on thermal destruction, has clearance limited by:- Thermal penetration depth (too shallow misses glands; too deep risks normal tissue)
- Individual variation in apocrine gland distribution
- Sections that cannot be visually verified
Literature shows greater variability in laser clearance rates, tied to operator experience, device parameters, and the patient's gland distribution.
This doesn't mean "laser is bad" — it's a structural difference between the two mechanisms on the "thoroughness" dimension. For patients aiming to handle the issue once and not revisit it, the direct-vision mechanism offers greater controllability.
Dimension 4: Recurrence Rate — 15-Year Follow-Up vs Literature
The rotational curettage technique has been performed at the clinic for 20 years, with no recurrence reported in 15 years of clinical follow-up to date (per clinic records; individual results may vary). The low recurrence rate is directly tied to high clearance — when apocrine glands are removed thoroughly, there is no residual tissue to resume secretion.
Laser bromhidrosis surgery shows higher recurrence in the literature, mainly not because "laser is flawed" but because completeness of clearance is limited by thermal penetration. Apocrine glands not fully destroyed may recover secretory function, with smell potentially returning over years.
Meaningful recurrence assessment requires long-term follow-up. In the short term (within a year) the two procedures may look comparable; the divergence shows up at 5 and 10 years.
Dimension 5: Recovery — Largely Similar
The two procedures are very close on this dimension:
- Procedure format: Both are same-day outpatient (local anesthesia, 1.5–2 hours)
- Pressure dressing: Both require about 7 days of pressure bandaging post-op to help the skin flap settle
- Recovery pace: Activity restriction in weeks 1–2 (no overhead arm motion, no weight training); daily activity in 3–4 weeks; most sports back by 1 month
Differences: rotational curettage involves a wider lifted flap, so early bruising can be more visible (usually fades by day 7–14); laser, due to thermal action, can produce more noticeable short-term skin sensation changes or burning sensations in some patients.
The "discomfort profile" differs slightly between the two, but overall recovery timelines are similar. Recovery period shouldn't be the primary factor in choosing between procedures.
Dimension 6: Cost — Reflecting Manual-Technique Density
Rotational curettage is usually more expensive because:- The direct-vision approach depends heavily on surgeon experience (clearance is judged by feel and visual cue)
- The procedure takes longer
- Equipment cost itself is lower; "technique value" makes up most of the cost
- The workflow is more standardized
- Equipment is more automated, with lower technique dependency
- But this also means outcome consistency is more sensitive to equipment and operator experience
The cost difference reflects "manual-technique density," not which one is "better value." When deciding, factor in the 5- to 10-year recurrence risk and possible re-treatment cost — not just the first procedure's price.
How to Choose — A Reference for Use Cases
Neither procedure is universally better; the choice depends on what you prioritize:
Lean toward rotational curettage if you:- Want one definitive procedure and would rather not undergo a second
- Accept the higher cost tied to manual-technique dependency
- Value the long-term low-recurrence record
- Have a strong family history (denser apocrine distribution)
- Are more cost-sensitive
- Have more localized gland distribution
- Are willing to accept a higher long-term recurrence possibility
- Have more flexibility on completeness of clearance
The final decision isn't "which is better" but "which fits your priorities." An in-clinic evaluation of your gland distribution, family history, and lifestyle needs gives the most useful basis for the choice.
FAQ
Is laser bromhidrosis surgery less painful?
Both are done under local anesthesia, so intraoperative pain is controlled in both cases. The post-op discomfort profile differs slightly: rotational curettage tends toward bruising and tightness; laser tends toward skin-sensation changes or burning sensation. Overall pain intensity is similar — the "laser is painless, curettage hurts" framing is not accurate.
I had laser surgery but the result was unsatisfactory — can I have rotational curettage afterward?
It can be evaluated. When apocrine activity remains after laser, rotational curettage as a secondary procedure is a common path. But the lifted-flap condition and scar tissue distribution affect technical difficulty, so an in-person evaluation of skin condition is needed to judge suitability and expected clearance.
Why does the clinic mainly recommend rotational curettage rather than laser?
Not because "laser is bad," but because the two mechanisms differ structurally on completeness. The clinic has spent 20 years on the rotational curettage technique, with over 10,000 cases, pursuing complete apocrine gland clearance as the goal via "thorough removal under direct vision." Laser suits some patients, but for those wanting "one definitive treatment," the direct-vision controllability of rotational curettage is the core advantage.
Will rotational curettage leave a scar?
Any skin incision leaves some scar. The rotational curettage incision is about 4mm; in most patients the scar fades over 3–6 months into a thin line close to skin tone. Scar appearance varies a lot by individual biology — keloid tendency, post-op wound care, skin tension all affect the final look. Pre-op evaluation provides care recommendations tailored to your skin.
What if there's still a sweat smell after surgery?
Once apocrine glands are removed, the "bromhidrosis smell" (the distinctive pungent note) is greatly reduced. But eccrine glands still produce sweat in the underarm, so a "sweat smell" (the regular sour sweat note) may persist — different smell source, different treatment path. If post-op sweat odor is bothersome, antiperspirants or Botox for sweat reduction can be considered, with no conflict with the bromhidrosis surgery.
Related Reading
- Sweat Gland Surgery: Curettage vs Laser vs miraDry vs ETS
- Bromhidrosis Surgery vs miraDry: A 6-Point Comparison
- Underarm Odor: Antiperspirant vs Botox vs Surgery
- Underarm Odor Surgery Aftercare: Recovery & Scar Care
- Axillary Bromhidrosis
Conclusion
Rotational curettage and laser are two different mechanisms for bromhidrosis surgery:
- Rotational curettage: mechanical removal under direct vision, high clearance, low recurrence, high technique dependency, higher cost
- Laser: thermal destruction, more standardized, lower cost, higher long-term recurrence
Choosing isn't about "which is better" but "which fits your priorities." If you're comparing the two and would like a doctor to evaluate your gland distribution and family history before choosing, a consultation may be worthwhile. Dr. Ta-Ju Liu has spent 20 years dedicated to axillary bromhidrosis treatment, with over 10,000 cases, and can help you clarify which approach fits you.
Related Reading
- Sweat Gland Surgery: Curettage vs Laser vs miraDry vs ETS
- Bromhidrosis Surgery vs miraDry: A 6-Point Comparison
- Underarm Odor: Antiperspirant vs Botox vs Surgery
- Underarm Odor Surgery Aftercare: Recovery & Scar Care
- Axillary Bromhidrosis
This article is educational. Individual results may vary; actual treatment requires in-person evaluation by Dr. Ta-Ju Liu.