Why Start with a Severity Self-Check
Hyperhidrosis isn't simply "I sweat more than average." The real medical question is: is the sweat clearly interfering with your life? A construction worker who sweats a lot may not have hyperhidrosis. An office worker in air conditioning who has to wipe their hand before every handshake might.
Many people delay seeing a doctor because "I don't know if I'm severe enough" or "maybe I'm overthinking it." This article gives you a 5-question self-check to sort yourself into mild, moderate, or severe — each with a matching treatment path. Not everyone needs surgery, but every level has something appropriate.
The 5-Question Self-Check (Yes/No)
Answer based on your normal pattern over the past 6 months — not your worst day.
| Question | Yes | No |
|---|---|---|
| Q1 Do your palms / armpits sweat even when you're neither hot nor anxious? | □ | □ |
| Q2 Does sweating affect your work? (paper getting damp, keyboard slipping, wiping hand before handshake) | □ | □ |
| Q3 Do you need to change clothes 2+ times within a day? | □ | □ |
| Q4 Do you avoid certain situations because of sweat? (public speaking, dates, gym class) | □ | □ |
| Q5 Have 2+ different antiperspirants given you only limited results? | □ | □ |
Count your yes answers:
- 0–1 yes: Mild
- 2–3 yes: Moderate
- 4–5 yes: Severe
What Each Level Means
Mild (0–1 yes): Manageable at the Lifestyle Level
This level means your sweating is within a reasonable context — heat, exercise, anxiety make you sweat more, but it isn't disrupting work or social life. First-line measures live at the lifestyle level:
- Fabric choice: cotton, linen, Coolmax — moisture-wicking fast-drying materials
- OTC antiperspirants: aluminum chloride products from the drugstore, applied at night, rinsed in the morning
- Avoid triggers: spicy food, caffeine, alcohol all increase sweating
- Weight management: higher BMI generally correlates with more sweating
The mild group usually doesn't need medical intervention. If you've already adjusted lifestyle but sweating is creeping up or starting to affect work, you can step up to evaluation later.
Moderate (2–3 yes): Consider Stronger Antiperspirants or Botox
This level means sweating is starting to interfere with daily life — wiping before handshakes, sweat marks on shirts, getting distracted in meetings worrying about visible sweat. First-line measures can be reinforced:
| Approach | Best for | Note |
|---|---|---|
| Prescription-grade antiperspirant | Armpits, palms | 20–25% aluminum chloride; higher skin irritation risk |
| Iontophoresis | Palms, soles | Multiple sessions needed; effect lasts 2–4 weeks |
| Botox injection | Armpits, palms | Effect lasts 4–6 months; needs repeat |
A common moderate-level blind spot is "I'll just push through with stronger antiperspirants." If a prescription-grade option doesn't show meaningful improvement after 4–6 weeks, an in-clinic evaluation for botox or alternatives is reasonable. Don't keep stacking concentration — high aluminum chloride can trigger contact dermatitis and make things worse.
Severe (4–5 yes): Book an Evaluation, Surgery on the Table
This level means sweating is clearly affecting work, social life, and emotional state — avoiding handshakes, avoiding public speaking, frequent clothing changes, long-term hits to confidence. The treatment path usually involves medical intervention:
- Step 1: Confirm the type in clinic — primary (no other underlying cause) vs. secondary (hyperthyroidism, diabetes, infection, etc.). Secondary cases need the underlying condition addressed first.
- Step 2: Botox injection — most severe-level patients start their medical intervention with botox: predictable effect, low risk, but needs repeat sessions.
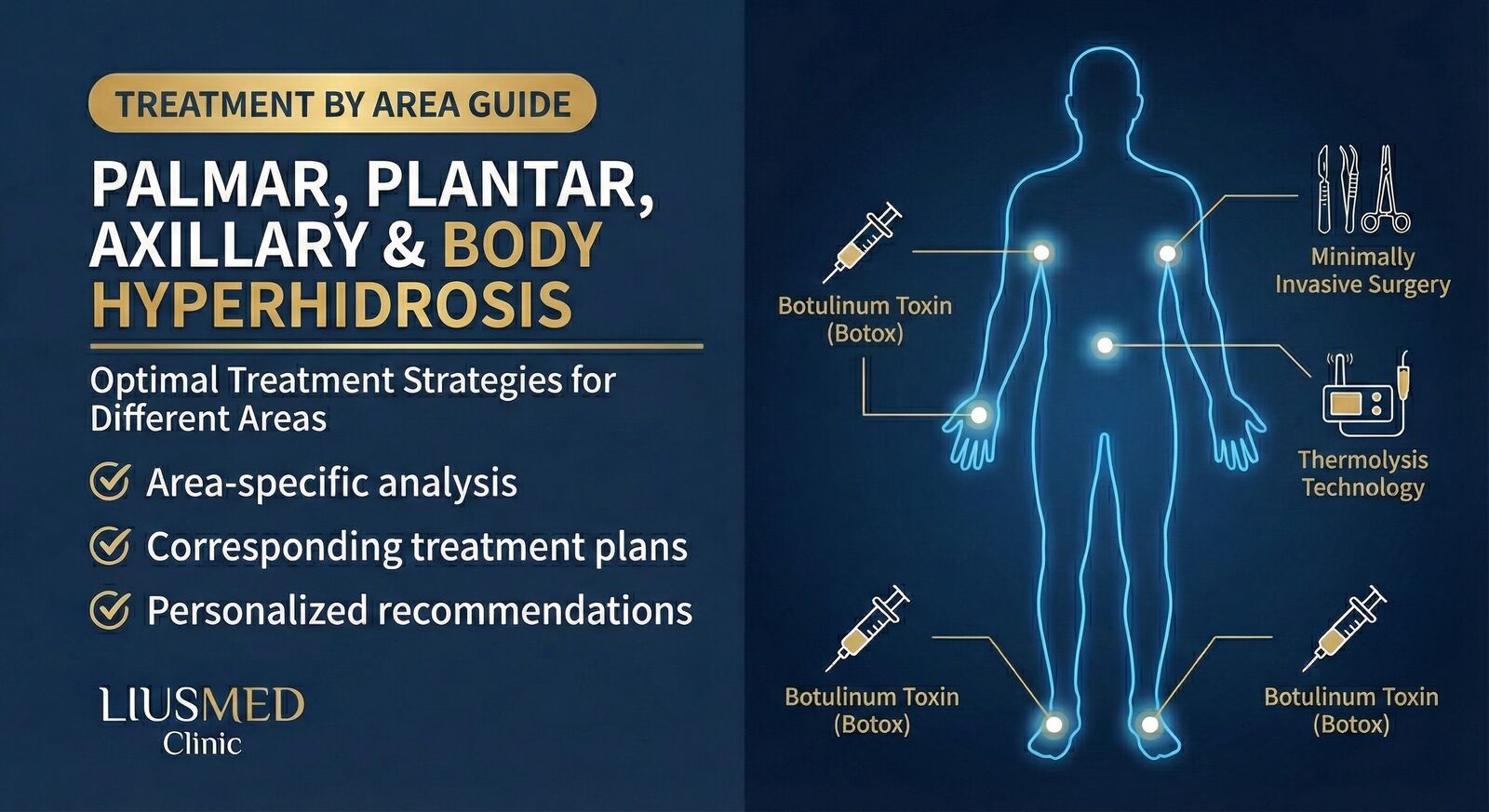
- Step 3: Surgical options — if botox results are insufficient or you don't want repeated injections, options include micro rotational curettage (for axillary severe sweating + bromhidrosis treated together) or endoscopic thoracic sympathectomy (ETS) (for palmar hyperhidrosis, but with compensatory sweating risk that needs full counseling).
Dr. Ta-Ju Liu has worked with axillary hyperhidrosis and bromhidrosis cases for over 20 years, with over 10,000 cases on record, and can help you compare treatment options against your situation. Individual results may vary.
A Single Table for All Three Levels
| Level | Yes count | First-line | Second-line |
|---|---|---|---|
| Mild | 0–1 | Fabric + OTC antiperspirant + lifestyle | Observation |
| Moderate | 2–3 | Prescription-grade antiperspirant / iontophoresis | Botox injection |
| Severe | 4–5 | Botox injection | Surgical evaluation (micro rotational curettage / ETS) |
A Few Extra Signals Beyond the Self-Check
The 5 questions cover the main direction. The following extra signals warrant earlier medical evaluation:
- Clear one-sided asymmetry (a lot of sweat on one side, normal on the other) → possible neurological cause
- Sudden worsening within 6 months (was fine before, much worse recently) → rule out secondary causes
- Accompanied by clear weight loss, palpitations, hand tremor → rule out thyroid issues
- Night sweats + fever + weight loss → rule out infection or systemic disease
These signals take higher priority than the sweating itself — the underlying cause needs to be ruled out before treating the sweat symptom.
FAQ
I scored 3 yes — moderate. Do I have to get botox?
No. The first-line for moderate is still prescription-grade antiperspirant or iontophoresis — try those for 4–6 weeks first. Botox is an option when first-line measures don't deliver enough improvement — moderate doesn't auto-route into botox. Before deciding on botox, weigh: re-injection cadence (every 4–6 months long-term), injection-site pain, rare side effects.
I have severe palmar sweating. I read online that ETS causes compensatory sweating — is that real?
Yes, it's real. Compensatory sweating after endoscopic thoracic sympathectomy (ETS) isn't rare — once palmar sweating drops, the body may compensate by sweating more on the back, lower back, or thighs; in some cases the compensatory area becomes more bothersome than the original palm sweat. So ETS isn't a "got palm sweat → operate" decision — it requires thorough counseling, full risk understanding, and ideally trying reversible options like botox first.
Drugstore antiperspirants give me red, itchy skin. What now?
You're sensitive to that ingredient (usually aluminum chloride). Options: 1) try a lower-concentration version, 2) switch to potassium alum natural products, 3) apply at night and rinse in the morning, 4) if none of these help, get an in-clinic botox evaluation (avoids skin contact irritation entirely). Don't push through the redness and itch — you can trigger contact dermatitis and make things worse.
Will hyperhidrosis improve on its own?
Primary hyperhidrosis usually doesn't resolve spontaneously — it appears at puberty, stays for life, may slightly decrease with age but doesn't disappear. Secondary hyperhidrosis (alongside other conditions) can improve once the underlying disease is treated. So if you're 30 and still significantly sweating, "wait and see" generally won't bring improvement.
Can hyperhidrosis and bromhidrosis be treated in one go?
Yes. Axillary hyperhidrosis and bromhidrosis often coexist — surgery to remove the apocrine glands (the bromhidrosis source) also removes a portion of the eccrine glands (the sweating source). So micro rotational curettage can be a one-procedure option for the "armpit sweating + bromhidrosis" group. That said, this is one option after medical evaluation, not an automatic recommendation.
Related Reading
- Bromhidrosis & Sweat Treatment: How to Choose What Fits You
- Sweating by Area: Palms, Underarms & Feet Treatment
- Why Palms Sweat: Primary vs Secondary & a Severity Check
- Hyperhidrosis & Compensatory Sweating
Conclusion
The treatment path for hyperhidrosis depends on severity:
- Mild: lifestyle + OTC antiperspirant is enough; no medical intervention needed
- Moderate: prescription-grade antiperspirant or iontophoresis; step up to botox if results fall short
- Severe: in-clinic evaluation recommended; botox is the typical first medical step; surgery is an option for longer-term plans
If your 5-question self-check lands in the moderate or severe range, or you're seeing signals like "sudden 6-month worsening" or "clear one-sided asymmetry," booking an evaluation is reasonable. Dr. Ta-Ju Liu has spent 20+ years on axillary hyperhidrosis and bromhidrosis treatment and can help clarify the type and the options.
Related Reading
- Sweating by Area: Palms, Underarms & Feet Treatment
- Why Palms Sweat: Primary vs Secondary & a Severity Check
- Sweaty Palms: 3 FDA-Approved Non-Surgical Treatments
- Hyperhidrosis & Compensatory Sweating
This article is educational. Individual results may vary; actual treatment requires in-person evaluation by Dr. Ta-Ju Liu.