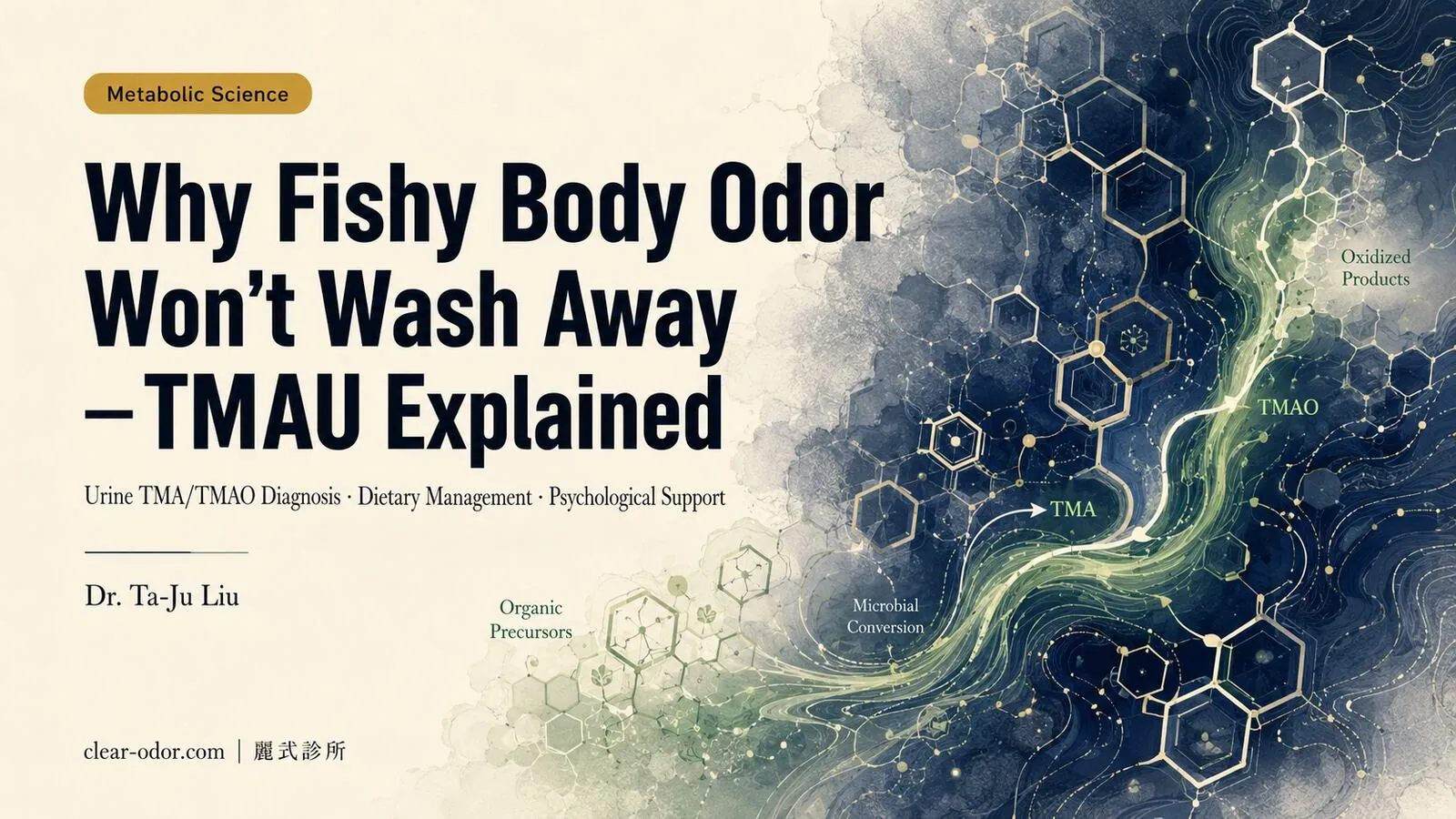

Fishy Odor, No Hygiene Link — This Is Not a Habit Problem
At the Integrated Odor Clinic, we occasionally encounter cases that are both puzzling and quietly difficult to live with.
A patient once described years of changing clothes twice daily, cycling through different body washes, and gradually withdrawing from social situations — and yet the persistent fishy odor never really went away. She had consulted dermatology and tried traditional remedies, with no clear explanation offered. A metabolic workup eventually confirmed trimethylaminuria (TMAU) — the entire journey had taken more than three years.
That kind of diagnostic delay is not unusual in TMAU.
TMAU is not a hygiene problem. It is not a psychological condition. It is a specific enzyme deficiency in a metabolic pathway. The role of the Integrated Odor Clinic in TMAU is to identify clinical clues, establish a referral pathway, and provide downstream education and psychological support — not to treat the underlying metabolic condition itself.Mechanism: FMO3 Enzyme and the Trimethylamine Pathway
Trimethylamine (TMA) is generated when intestinal bacteria metabolize choline-containing foods. In a healthy metabolic pathway, TMA absorbed into the bloodstream is oxidized by the hepatic enzyme FMO3 (flavin-containing monooxygenase 3) into odorless trimethylamine N-oxide (TMAO), which is then renally excreted.
In TMAU, the FMO3 gene (chromosome 1q24.3, OMIM #602079) carries mutations or has reduced expression, so TMA cannot be adequately converted. Free TMA accumulates and is excreted through sweat, breath, and urine — producing a persistent fishy odor with essentially no correlation to how often one washes.
The inheritance pattern is primarily autosomal recessive. A minority of cases are secondary TMAU (gut microbiome dysbiosis causing excess TMA production) or transient (triggered by infection, menstruation, or a high-choline dietary episode).
| Type | Mechanism |
|---|---|
| Primary (genetic) | FMO3 biallelic mutations → persistent enzyme deficiency |
| Secondary | Excess intestinal TMA production exceeding FMO3 capacity |
| Transient | Infection, menstruation, or a large choline load as triggers |
Reference: Cashman JR & Zhang J (2006), Molecular Pharmacology 69(4), FMO3 functional review; OMIM #602079.
Diagnosis: Urine TMA/TMAO Ratio and Genotyping
Urine TMA/TMAO Ratio (Core Diagnostic Indicator)
- Normal: TMAO accounts for 85–95% of total urinary trimethylamine (nearly all TMA oxidized to odorless form)
- TMAU patients: Free TMA fraction significantly elevated — often >20%, severe cases >50%
- Collection protocol: Urine collected 8–12 hours after a TMA-precursor challenge meal (typically a fish-heavy serving), analyzed by GC-MS
Genotyping
Confirming FMO3 mutation sites (common SNPs: N61S, E158K, E308G) helps establish genetic TMAU, assess family risk, and guide subsequent treatment decisions.
Differential: TMAU vs. Apocrine Bromhidrosis
| Feature | TMAU Fishy Odor | Apocrine Bromhidrosis |
|---|---|---|
| Odor character | Persistent fishy odor, little correlation with hygiene | Axillary or localized, worsens after activity |
| Dietary link | Clearly amplified by high-choline foods | Not prominent |
| Diagnostic tool | Urine TMA/TMAO ratio + genotyping | Physical exam and history |
| Treating specialty | Metabolism / Genetics | Dermatologic surgery / Odor clinic |
When TMAU is suspected, referral to metabolism or genetics for formal testing is the appropriate pathway — not dermatologic surgery.
Clinical Note
If your body odor has a persistent fishy character, is disproportionate to your hygiene routine, and tends to worsen after eating eggs, fish, or legumes — discuss metabolic screening with a physician. Significantly restricting your diet without a confirmed diagnosis risks inadequate intake of essential nutrients.
For the broader framework of systemic metabolic body odor, see the Comprehensive Guide to Systemic Metabolic Odor.
Dietary Management: Four Precursor Categories to Restrict
Dietary adjustment is currently the most central and actionable daily management strategy for TMAU (Cashman & Zhang 2006). The principle is to reduce intestinal TMA production so that residual FMO3 activity can maintain free TMA at a lower concentration.Category 1: Choline-Containing Foods
Choline is the primary TMA precursor. Certain gut bacteria (particularly Clostridium species) convert it to TMA.
| High-Choline Food | Choline Content (per 100g, approx.) |
|---|---|
| Egg yolk | ~680 mg |
| Beef / pork liver | ~420–430 mg |
| Shellfish (oysters, clams) | ~65–200 mg |
| Whole soybeans | ~115 mg |
| Peanut butter | ~62 mg |
Note: The choline values above are approximate estimates from food-composition databases (e.g., USDA FoodData Central), intended for relative comparison only; their source differs from the FMO3-mechanism reference (Cashman & Zhang 2006) cited earlier.
The clinical recommendation is typically to significantly reduce frequency and portion size — not to eliminate entirely. Choline is an essential nutrient (neurotransmitter synthesis, cell membrane integrity); pregnant patients with TMAU particularly need individualized guidance from a metabolic specialist to avoid any impact on fetal neural development.
Category 2: Lecithin (Phosphatidylcholine)
Lecithin is also converted to TMA by gut bacteria. Common sources: soy lecithin supplements (widely sold health products), food emulsifiers (additive E322), eggs, and soy-based foods.
Many TMAU patients are unknowingly taking lecithin supplements — this is one of the most common hidden triggers of unexplained symptom flare-ups, and the one most easily overlooked.
Category 3: Direct TMA Sources (Marine Fish and Cured Seafood)
Certain sea fish, crustaceans (shrimp, crab), and fermented or cured seafood already contain preformed free TMA. Consuming them adds directly to the body's TMA load — sometimes more acutely than high-choline foods. Salted fish and fermented shrimp paste are especially notable.
Category 4: L-Carnitine
L-carnitine can also be metabolized to TMA by specific gut bacteria, though individual variation is considerable. Sources include red meat (beef, lamb) and L-carnitine supplements. Under specialist guidance, patients may consider moderately reducing intake.
Adjunct Interventions
All of the following require evaluation by a metabolism specialist or relevant physician before use. The Integrated Odor Clinic provides referral pathways, not metabolic prescriptions:
- Short-course gut antibiotics (metronidazole or rifaximin): suppress TMA-producing intestinal bacteria; typically a diagnostic therapeutic trial, effects are transient, requires specialist supervision.
- Riboflavin (vitamin B2) supplementation: FMO3 is a flavoenzyme; some evidence suggests moderate supplementation supports residual FMO3 activity. Relatively safe, but efficacy varies by mutation site.
- Oral activated charcoal: transiently adsorbs intestinal TMA; adjunctive use only — long-term use may impair absorption of fat-soluble vitamins and minerals.
- Probiotic microbiome modulation: human trial data remain limited; specific Lactobacillus strains may reduce TMA production as an adjunct, but this is not yet a standard treatment recommendation.
Psychological Support: The Chronically Underestimated Dimension
The psychological burden of TMAU is severely underrecognized in clinical practice.
Years of unexplained fishy odor, being misread as having poor hygiene, repeated consultations yielding no diagnosis — these compound into: social withdrawal (avoiding work and relationships), generalized anxiety or depression, and in some cases features of olfactory reference syndrome (ORS) — continuing to fear the odor even after it is well-controlled.
Research by Lomholt & Mikkelsen (2011) found that most TMAU patients experienced significant emotional distress during the diagnostic delay period, with some reporting self-harm or suicidal ideation. Receiving a diagnosis is itself an important milestone — shifting the frame from "it's my failing, my bad habits" to "this is a named physiological condition."
Key Points for Integrated Psychological Support
- Psychologist or psychiatrist evaluation: CBT for co-occurring anxiety, depression, or ORS features
- Family and workplace empathy education: helping those around the patient understand TMAU as a metabolic condition, not a hygiene failure
- Peer support networks: international TMAU Support Groups (online communities); in Taiwan, the Foundation for Rare Disorders offers some resources and contacts
Role of the Integrated Odor Clinic: Screening + Referral
In the Comprehensive Guide to Systemic Metabolic Body Odor, we outlined the full picture: this category of odor exceeds the scope of dermatologic surgery, and the Integrated Odor Clinic's defined role is screening plus referral — not primary management of systemic disease.
TMAU is the clearest example of this boundary. If you suspect TMAU:
- Start with an initial consultation at the Systemic/Metabolic Odor Integrated Clinic — to rule out common causes and establish clinical clues
- Referral to metabolism or genetics for urine TMA/TMAO ratio testing and FMO3 genotyping
- After confirmed diagnosis, return to the integrated clinic to coordinate dietary education, psychological referral, and a life-management plan
- Book a consultation
Frequently Asked Questions
Can TMAU (fish odor syndrome) be passed on to the next generation?
It's mainly autosomal recessive: usually both parents each carry an FMO3 gene variant before a child is likely to be affected. Genotyping can help assess the risk for family members.
Can TMAU be cured?
At present the FMO3 gene itself cannot be changed, so TMAU cannot be cured in that sense. But with dietary management and adjunct interventions, most people can keep the fishy odor at a lower level. The clinical goal is long-term, stable management rather than a one-time fix.
How can I tell whether I have TMAU or ordinary bromhidrosis?
TMAU produces a persistent fishy odor with little relation to how often you wash, and it tends to worsen after eating eggs, fish, or legumes. Apocrine-type bromhidrosis is usually concentrated in the underarms and worsens after activity. To distinguish them definitively, you need a urine TMA/TMAO ratio test.
Why don't constant showering and antibacterial soap help?
Because trimethylamine comes from metabolism inside the body, not from bacteria on the skin surface, so cleaning the skin makes limited difference. The key is reducing intake of precursor foods and managing things on the metabolic side.
If I suspect TMAU, should I see dermatology or metabolism first?
We recommend referral to metabolism or genetics for formal testing. The Integrated Odor Clinic can do an initial consultation first, rule out common causes of body odor, and help establish a referral pathway for you.
Do I have to cut out eggs and seafood entirely?
Completely eliminating them on your own isn't advisable. The approach is to significantly reduce frequency and portion size, with individualized assessment by a specialist, so you don't fall short on essential nutrients such as choline (pregnant patients especially need specialist assessment).
Related Reading
- Whole-Body Metabolic Odor: TMAU, Diabetes & Liver Signals
- Sudden Strange Body Odor or Breath? 5 Disease Red Flags
- Not Bromhidrosis but Whole Body Smells? Where to Start
- Bad Breath Despite Brushing? It's Usually Not Your Stomach
- Systemic / Metabolic Odor Screening
Conclusion
TMAU (trimethylaminuria) is a genetic metabolic condition in which FMO3 enzyme deficiency causes persistent fishy body odor — with a pathological mechanism entirely distinct from apocrine bromhidrosis. Diagnosis depends on urine TMA/TMAO ratio and genotyping; dietary management (restricting choline, lecithin, direct TMA sources, and L-carnitine) is the most actionable daily strategy; and psychological support is an equally important dimension that is too often overlooked.
The Integrated Odor Clinic's role here is to provide the screening clues and referral pathway — and clarity about that role is what enables patients to find genuinely effective help.
Dr. Ta-Ju Liu / Integrated Odor Clinic