
Scalp Odor Integrated Assessment: From Microbiome to Medical Intervention
Sebum × Malassezia × Bacteria Three-Layer Analysis + Stepped Personalized Plan
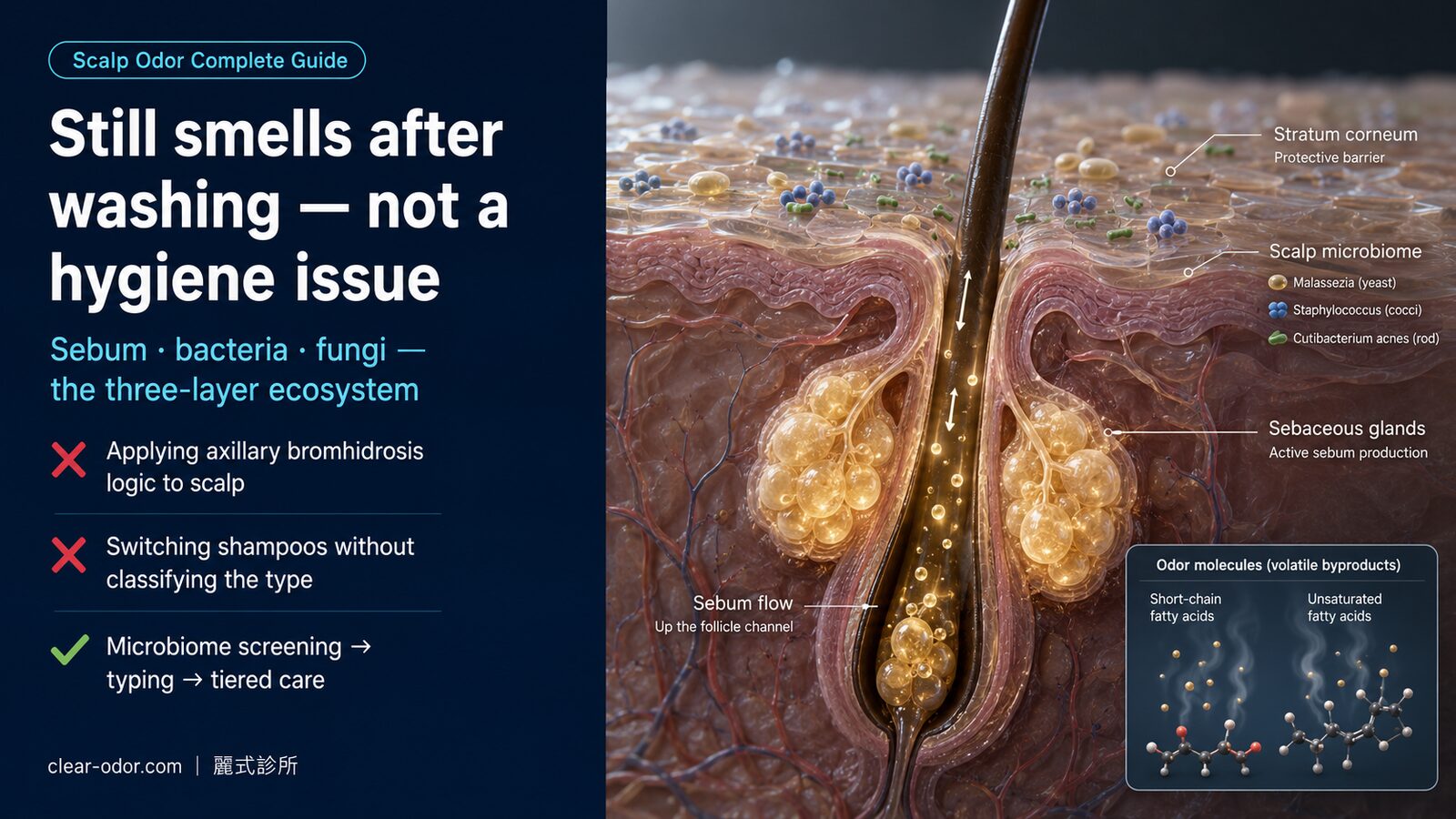
Scalp odor differs fundamentally from underarm or intimate-area "apocrine gland" odor — the scalp has very few apocrine glands. The dominant cause is the extremely high density of sebaceous glands (300-900 per cm²), whose triglyceride secretions are metabolized by surface bacteria (Staphylococcus, Cutibacterium) and fungi (Malassezia restricta / globosa) into short-chain and unsaturated fatty acids. Liu's Integrated Odor Clinic offers a stepped "home protocol → medical intervention → advanced assessment" approach to identify root causes and progressively reduce odor.
Table of Contents
Why Does My Scalp Still Smell After Washing?
Scalp malodor is common in dermatology practice but often underestimated. Its mechanism differs from underarm or areola bromhidrosis — those are driven by apocrine glands, whereas the scalp has almost none. The dominant driver is microbial imbalance on a scalp that produces large volumes of sebum.
Want to compare odor management across other body sites? See body odor & hyperhidrosis conditions overview to compare definitions, ICD-10 codes, symptoms, and when to see a doctor.
Why a few hours after washing, the smell returns
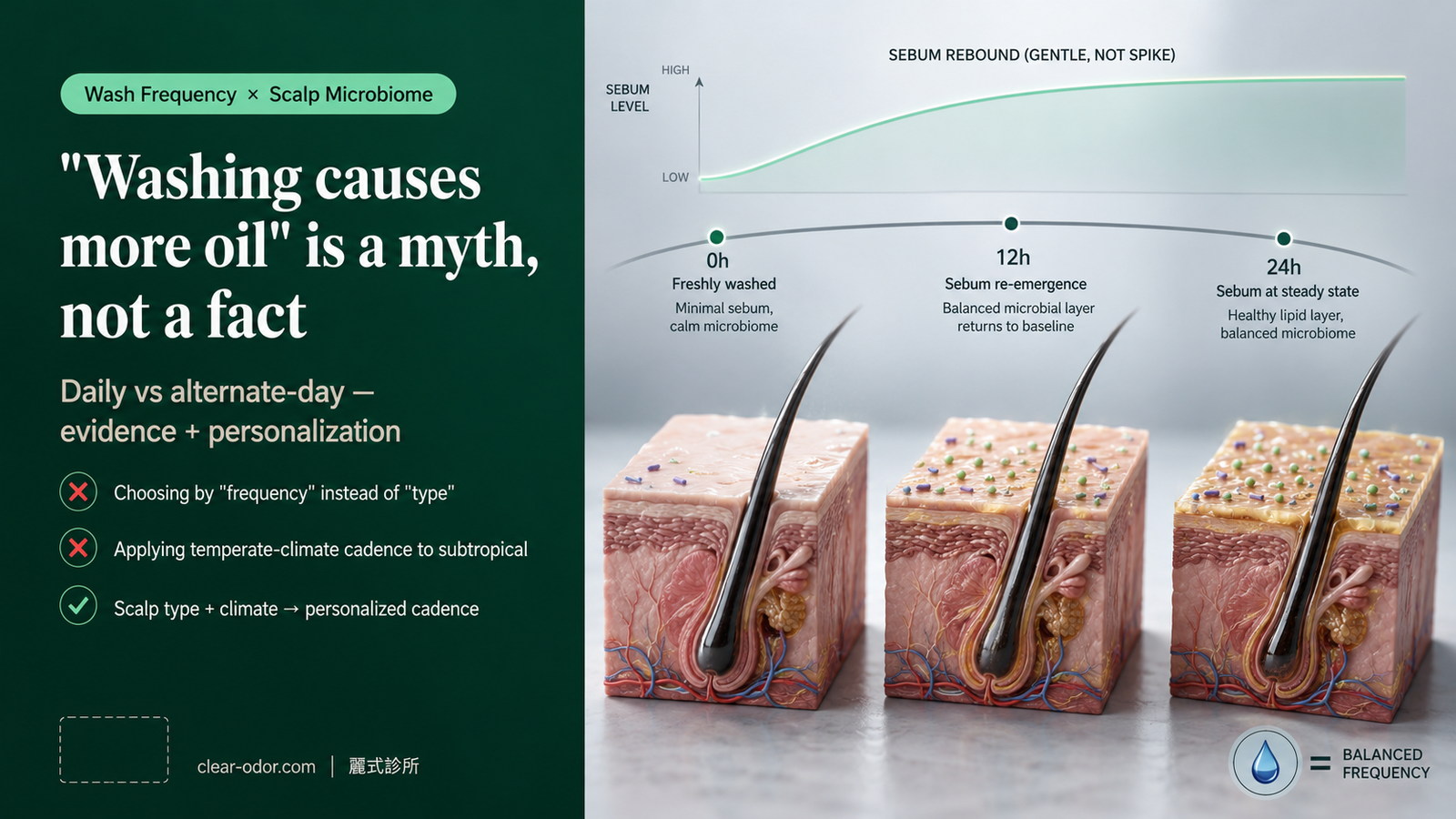
Sebum production typically rebounds within 2-6 hours of washing. When sebum triglycerides are broken down by bacterial lipases into short-chain fatty acids (propionic, butyric), and Malassezia fungi produce unsaturated fatty acids (e.g., oleic acid), the result is a sour/oily smell — usually most noticeable during exercise, stress, hat-wearing, or when the scalp gets warm and humid.
Why "integrated assessment" rather than just switching shampoo
Switching shampoo alone often misses: (1) whether the odor is from sebum metabolism, Malassezia overgrowth, or seborrheic dermatitis; (2) amplifiers like diet, hormones, and stress; (3) the gap between perceived vs. observed odor (a small subset falls into olfactory reference territory). Integrated assessment unpacks each layer.
Three-Layer Scalp Microbiome Analysis
Our integrated clinic evaluates the scalp in three layers — which layer is imbalanced determines the next step: adjust hygiene cadence, add antifungal medication, or run advanced microbiome testing.
Layer 1: Sebaceous Glands
Scalp sebaceous gland density (300-900/cm²) is second only to the T-zone. Regulated by androgens, diet, and stress. Sebum itself is odorless, but it feeds the bacterial and fungal communities.
Layer 2: Bacterial Flora
Resident bacteria like Staphylococcus epidermidis and Cutibacterium acnes lipolyze sebum triglycerides into short-chain fatty acids — the primary source of the "sour" smell.
Layer 3: Malassezia Fungi
Lipid-dependent yeasts (particularly M. restricta, M. globosa) metabolize sebum into unsaturated fatty acids, closely linked to seborrheic dermatitis, dandruff, and a distinctive oily-rancid odor.
Clinical Reading
Odor + dandruff + erythema + itching → Layer 3 (Malassezia / seborrheic) is dominant. Odor + greasy sheen + folliculitis → Layers 1+2 (sebum + bacteria). Odor without visible skin changes that others don't notice → olfactory reference assessment may be appropriate.
4-Week Home Protocol
Before medical intervention, most scalp odor cases benefit from 4 weeks of systematic home care. Track odor intensity (self-rated 0-10) and accompanying symptoms (flakes, itch, oiliness) at weeks 0, 2, and 4.
Personalize Wash Frequency
Oily scalp: wash daily (avoid over-stripping that triggers rebound oiliness). Dry/neutral: every 2-3 days. Water temperature 38-40°C — hot water amplifies sebum production.
Use Active-Ingredient Shampoo
Antifungal: Zinc Pyrithione 1-2%, Ketoconazole 1%, Selenium Sulfide 1%. Keratolytic: Salicylic Acid 2-3%. Rotate to avoid tolerance.
Thorough Rinse + Double Cleanse
Let antifungal shampoo dwell 3-5 minutes before rinsing. Product residue (styling, conditioner) is a commonly overlooked odor source — rinse with water first, then shampoo twice.
Diet & Lifestyle
Reduce high-fat, refined sugar, alcohol. Add Omega-3 and zinc. Sleep 7+ hours. Manage stress (cortisol amplifies sebum production).
Avoid Amplifiers
Long-duration hats/helmets, unwashed sweat on scalp, shared towels and pillowcases, high-alcohol styling products (barrier damage). Change pillowcases weekly.
Medical Intervention Ladder (when 4-week home protocol fails)
Our integrated clinic intervenes in three tiers based on severity and microbiome assessment. The principle is "lowest necessary intensity, regular reassessment."
| Tier | Intervention | When to Use |
|---|---|---|
| Tier 1: Prescription Shampoo | Prescription-strength Ketoconazole 2%, Ciclopirox 1% antifungal cleansers | After 4-week home protocol — persistent oily-rancid odor + mild dandruff |
| Tier 2: Short-term Topical Therapy | Low-potency topical steroid (short course for acute seborrheic flares), topical calcineurin inhibitors (sensitive skin) | Accompanied by visible erythema, itching, dandruff |
| Tier 3: Advanced Assessment | Microbiome panel (flora analysis), sebum analysis, oral antifungals (severe/refractory), laser/photobiomodulation for sebum modulation | 8 weeks of Tier 1+2 with no improvement, or recurrent relapse |
* All medical interventions are individualized based on clinical assessment; results may vary. This clinic does NOT advocate applying apocrine gland surgery to scalp odor — literature support is extremely limited. Such discussion is reserved for the rare case of imaging or biopsy confirming aberrant apocrine distribution.
When to See the Integrated Odor Clinic
If any of the following apply, book an integrated assessment rather than trying yet another shampoo:
- < 30% improvement after 4 weeks of systematic home protocol
- Accompanying hair loss, scalp erythema, visible dandruff, or itching
- Odor affects social, work, intimate life, or self-esteem
- You perceive strong odor but close contacts don't (olfactory reference assessment may be appropriate)
- Odor at multiple body sites (underarms, intimate, feet) needing integrated handling
The dedicated 30-45 min Odor Map Initial Consultation launches in Phase 2. For now, please book a general dermatology consultation.
About the Integrated Odor Clinic
Dr. Ta-Ju Liu
Dr. Ta-Ju Liu
Lead Physician, Clear Odor Integrated Odor Clinic
- 20 years of clinical experience in odor and sweat gland disorders
- Founder of Liu's Integrated Odor Clinic (scalp / oral / body / intimate / metabolic / OlRS)
- 10,000+ apocrine gland procedures across axillary, areola, and perineal sites
- Recent focus: multi-site integrated odor assessment and microbiome analysis
"Odor is rarely about one site — it's a signal from the body's interaction with its microbiome. Integrated assessment finds the root cause better than another shampoo bottle."
FAQ
Q1.Is scalp odor an extension of underarm "apocrine bromhidrosis"?
Q2.Can I just have apocrine surgery applied to my scalp?
Q3.I use anti-dandruff shampoo but the smell persists — am I doing it wrong?
Q4.Does diet really affect scalp odor?
Q5.Is scalp odor linked to stress?
Q6.I think I smell strongly, but family says I don't — what now?
Q7.Can scalp odor be "cured"?
Q8.When will the Odor Map Initial Consultation launch?
Related Services
Approach Scalp Odor as a Microbiome Signal
Not a shampoo problem — a layered diagnostic question. Book an integrated assessment to address root causes.
Book Integrated AssessmentCan't use LINE? Leave us your contact details
Replies within 1 hour during business hours — we only use this info to respond
Learn More About Scalp Odor
Scalp Odor After Washing? The Microbiome & How to Manage
Scalp odor isn't axillary bromhidrosis spreading upward. It's the product of a high-density sebaceous field (300-900 glands per cm²) whose secretions are metabolized by surface bacteria (Staphylococcus, Cutibacterium) and yeast (Malassezia restricta / globosa) into short-chain and unsaturated fatty acids. Dr. Ta-Ju Liu lays out 5 clinical archetypes, a 4-week home-care protocol, a Tier 1-3 medical intervention ladder, why we do not advocate transferring axillary sweat-gland surgery to the scalp, how to navigate the gray zone of Olfactory Reference Syndrome (OlRS), and how to pace 3 / 6 / 12-month maintenance check-ins.

Scalp Odor: Antifungal or Antibacterial Shampoo? 5 Signs
The most common reason people pick the wrong shampoo for scalp odor is not knowing whether they're dealing with seborrheic dermatitis (Malassezia-driven) or bacterial overgrowth — the first needs an antifungal, the second needs an antibacterial. This article walks through 5 quick-identification indicators, a self-check flow, the management path for each type, and how to handle the mixed type, so you can read your own scalp before choosing an OTC shampoo.
Wash Hair Daily or Every Other Day? Scalp Microbiome
'I heard that washing my hair every day will make my scalp oilier' is one of the most common myths I hear in the scalp-odor clinic. This article reviews the dermatology evidence on how wash frequency affects the scalp microbiome, sebum output, and Malassezia overgrowth — debunking the 'rebound oiliness' myth, offering a personalized framework for oily, normal, and dry scalps, and explaining why humid subtropical climates like Taiwan need a different washing rhythm than temperate regions.

Bromhidrosis & Sweat Treatment: How to Choose What Fits You
Facing the full spectrum of bromhidrosis, hyperhidrosis, and post-ETS compensatory sweating options, what most often paralyzes patients isn't 'which one is best,' but 'which one is best for me.' Dr. Ta-Ju Liu organizes a 5-dimension decision matrix (severity, timeline, budget, surgical tolerance, comorbidity), walks through 4 archetypal patient scenarios (17-year-old bullied teen / 32-year-old bride / 45-year-old man with combined odor + sweat / 22-year-old post-ETS), applies the 'Minimum Viable Treatment' principle, explains when to revisit the decision, and offers a consultation prep checklist. Designed to help you bring the right questions into the consultation room.
By age / cause axis
Only started after midlife — and will not wash off?
Aging odor × halitosis × systemic-metabolic — sort the source and the right specialist in the Midlife & Aging Odor guide
⚕️ Medical Disclaimer
The medical information provided on this page is for reference only and cannot replace individual face-to-face diagnosis, advice, or treatment from a physician. All medical procedures carry risks. Individual constitution and post-operative recovery vary from person to person. Please discuss any treatment plan with your attending physician before making decisions.