
Why You Need a Full Guide on Scalp Odor
Every week in clinic, I (Dr. Ta-Ju Liu) hear variations of the same three sentences:
- "I wash my hair every day, but by mid-afternoon it smells greasy — is it the shampoo?"
- "I read online that scalp odor is also bromhidrosis. Can surgery fix it?"
- "I think I smell bad, but my family says they can't smell anything. Is it just in my head?"
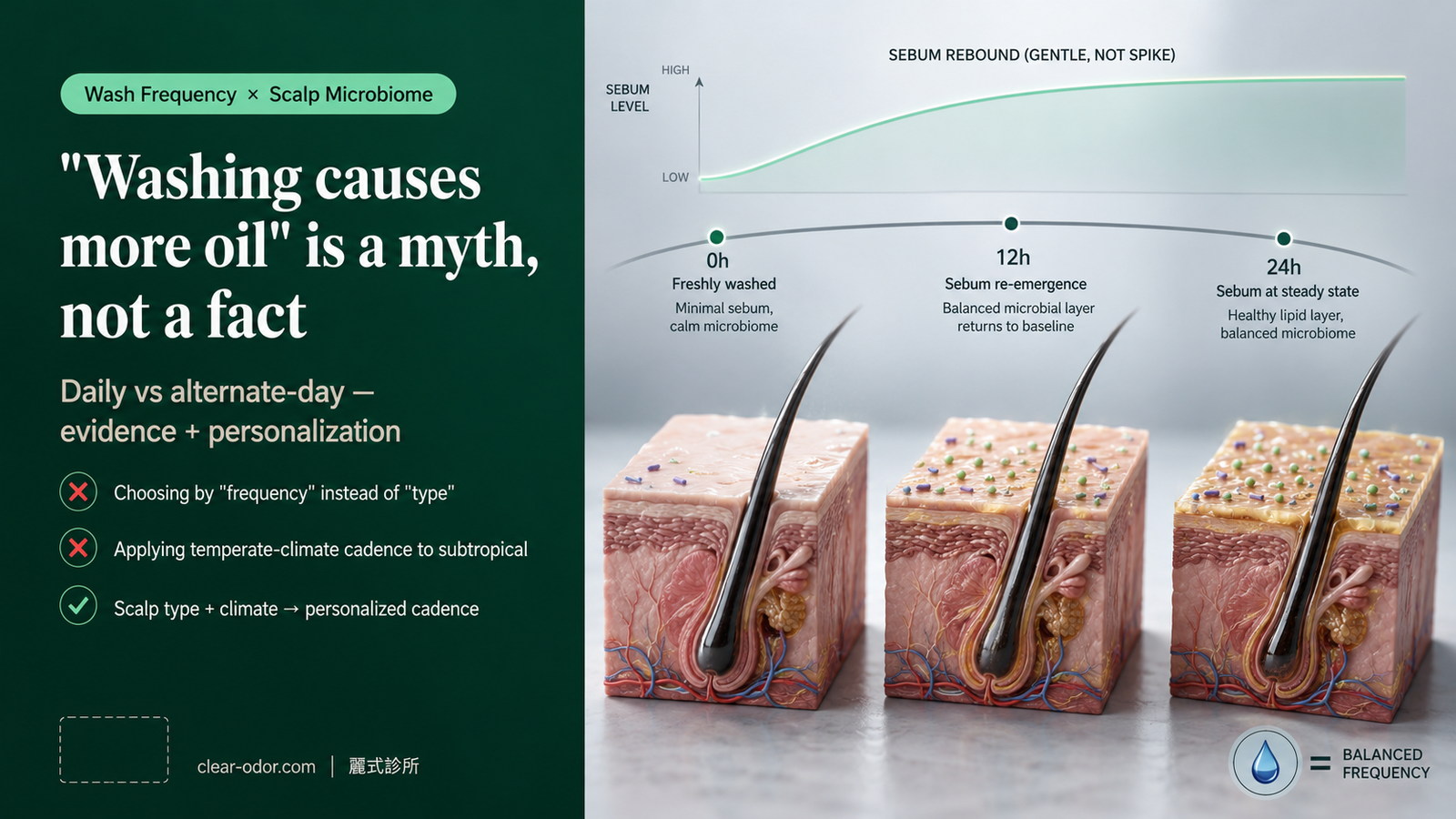
Behind these questions sits the same misunderstanding: the assumption that scalp odor works like axillary bromhidrosis, and that the right shampoo or the right surgery will solve it.
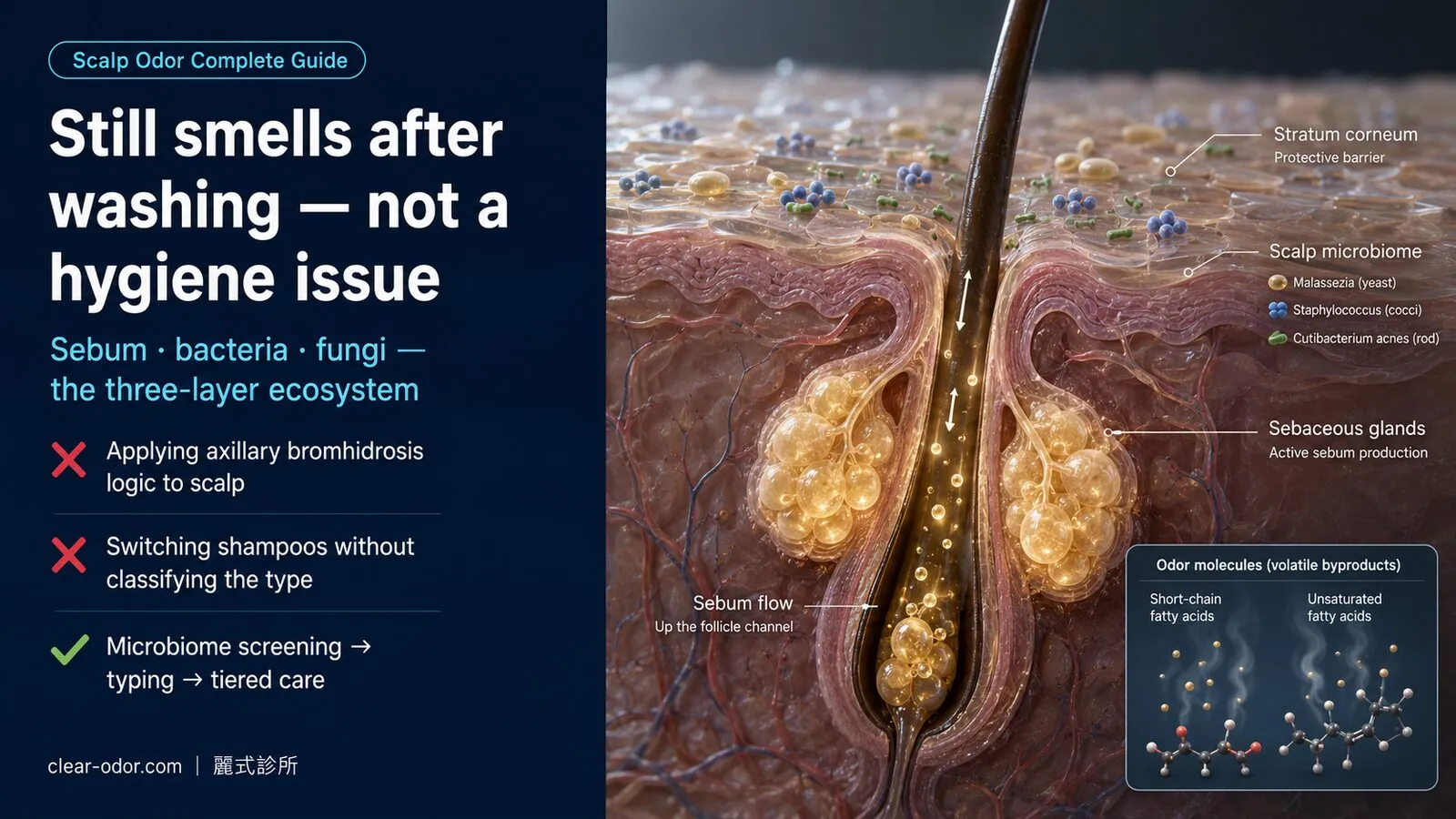
In reality, the scalp has almost no apocrine glands — the gland family responsible for odor in the underarms, areolae, and groin. High odor output from the scalp is driven by an extremely dense sebaceous field (300–900 glands per cm², second only to the T-zone) combined with microbiome imbalance. In other words, scalp odor is a signal of how your body and its microbes are interacting — it isn't a single-gland problem.
This guide consolidates the 20 years of clinic questions I get most often into a framework you can use before your consultation, so you can already see which type you fall into and where on the ladder to start. By the end you should be able to answer:
- Which clinical archetype of scalp odor do I fit?
- Which active ingredients work for me, and how do I use them so they keep working?
- When should I escalate to prescription therapy? When do I need advanced testing?
- Why doesn't Dr. Liu recommend applying axillary bromhidrosis surgery to the scalp?
- "I think I smell, but no one else does" — what do I do with that?
Individual results vary — this guide offers a decision framework, not a diagnosis. The final treatment plan still requires an in-person evaluation.
Multi-site odor? If you have odor in more than one area, see the Odor Map for site-by-site triage first to identify the primary source before diving into this guide.
How do scalp odor and underarm bromhidrosis differ mechanistically?
Scalp odor isn't "bromhidrosis spreading upward" — underarm bromhidrosis comes from apocrine glands, while scalp odor mainly comes from the interplay of sebaceous glands, bacteria, and fungi; different mechanisms, so treating scalp odor as B.O. (or wanting sweat-gland surgery) sends you down the wrong path.A lot of people misread scalp odor as "bromhidrosis spreading upward." It's a critical misconception, because it leads to choosing the wrong treatment path.
1. Apocrine-Type Odor (Axilla / Areola / Groin)
The main driver is apocrine glands, whose protein and lipid secretions are metabolized by specific bacteria (e.g., Corynebacterium) into short-chain fatty acids and thiol compounds. Hallmarks:
- Onset at puberty
- Restricted to specific regions (axilla, areola, groin, ear canal)
- Clearly linked to emotional state and sexual arousal
- Substantially improved by physical removal of apocrine glands (which is why surgery works for this category)
2. Scalp-Type Odor (Sebaceous-Driven)
The main driver is the triglycerides secreted by sebaceous glands, broken down by the lipases of resident bacteria (Staphylococcus epidermidis, Cutibacterium acnes) into short-chain fatty acids (propionic, butyric), with additional unsaturated fatty acids (e.g., oleic acid) generated by Malassezia yeasts — particularly M. restricta and M. globosa. Hallmarks:
- Occurs at any age (children to older adults)
- Recurs within 2–6 hours after shampooing
- Closely tied to diet, stress, hormones, and a hot occluded scalp
- Physically excising sebaceous glands carries far more risk than benefit (follicular damage, permanent alopecia)
3. Why Does This Distinction Matter So Much?
Because different mechanisms mean entirely different treatment paths. If you treat scalp odor as if it were bromhidrosis, you will:
- Seek out axillary bromhidrosis surgery for the scalp → the literature offers very limited support, and risks far exceed expected benefit
- Expect "one-time resolution, never to recur" → the microbiome is dynamically regulated; the realistic goal is to bring it down to a non-bothersome level and maintain it
- Overlook diet, stress, and washing frequency — the "actually modifiable" amplifiers
The first job at the Integrated Odor Clinic is to identify which dominant mechanism is driving your odor — not to pick a tool, but to read the problem correctly first.
How do you read the scalp microbiome? A three-layer (sebum × bacteria × fungus) analysis
The clinic evaluates the scalp in three layers: sebaceous glands (how oily), bacteria (breaking sebum and sweat into a musty-sour smell), and fungi (Malassezia causing rancid odor and seborrhea) — each layer offers a point to intervene, and understanding all three tells you which layer your odor needs.The Integrated Odor Clinic evaluates the scalp in three layers, each with its own intervention points.
Layer 1: Sebaceous Glands
Scalp sebaceous gland density (300–900 / cm²) is second only to the T-zone and is regulated by three main factors — androgens, diet, and stress:
- Androgens: Men and women with polycystic ovary syndrome (PCOS) tend to have higher sebum output
- Diet: High-fat foods, refined sugars, and alcohol amplify secretion; Omega-3 and zinc help normalize sebum composition
- Stress: Cortisol amplifies androgen-driven stimulation of sebaceous glands — this is the physiology behind "my scalp gets oilier right before exams"
Sebum itself is odorless, but it supplies the substrate for the next two layers. So simply washing sebum away is only a temporary reduction in fuel — secretion resumes within hours and the cycle restarts.
Layer 2: The Bacterial Community
Resident bacteria on the scalp (Staphylococcus epidermidis, Cutibacterium acnes, etc.) use lipases to cleave sebum triglycerides into free fatty acids. The short-chain fatty acids (C2–C6) are the primary source of the "sour" odor note.
Bacterial imbalance usually shows up as:
- Visible shine, follicular redness (folliculitis)
- An odor that leans "sour" and "stuffy"
- Good response to antibacterial actives (Zinc Pyrithione, Selenium Sulfide)
Layer 3: Malassezia Yeasts
Malassezia is a lipid-dependent yeast present on virtually every human scalp, but in overgrowth it:
- Converts saturated fatty acids in sebum into unsaturated fatty acids (e.g., oleic acid), irritating the scalp → seborrheic dermatitis, dandruff
- Generates the distinctive "greasy" and "musty" odor notes
Signs of Malassezia overgrowth: dandruff, erythema, itching, and a greasy odor appearing together. The matching treatment is antifungal, not antibacterial — which is why anti-dandruff shampoo sometimes outperforms a regular "oil-control" shampoo.
Clinical Reading Formula
| Primary presentation | Dominant layer | First-line approach |
|---|---|---|
| Shine + sour note + no dandruff | Layers 1 + 2 | Personalized wash frequency + Zinc Pyrithione |
| Greasy odor + dandruff + erythema | Layer 3 — Malassezia | Ketoconazole / Selenium Sulfide antifungal |
| Odor + hair loss + inflammation | Cross-layer + seborrheic dermatitis | Prescription therapy + short-term topical steroid |
| Self-perceived odor unconfirmed by others, normal skin | OlRS assessment needed | See Section 7 |
What are the 5 common clinical archetypes of scalp odor?
Five common archetypes: oily-sebum dominant, bacterial musty-sour dominant, Malassezia-seborrhea dominant, mixed, and a gray zone where you smell it but no objective source is found — matching yourself helps find which layer and direction to start with.Twenty years of clinic distilled scalp odor into 5 common archetypes. Matching yourself to one helps you find your starting point.
| Archetype | Typical presentation | Main mechanism | Starting approach |
|---|---|---|---|
| A. Oily + Bacterial-Dominant | Oily by midday, sour note, no dandruff | Layers 1 + 2 | Daily wash + Zinc Pyrithione 1–2% |
| B. Seborrheic Dermatitis Type | Greasy odor + dandruff + erythema + itch | Layer 3 — Malassezia | Ketoconazole 1% OTC, reassess at 4 weeks |
| C. Product-Residue Type | Odor worsens after heavy styling / conditioning | Product residue + bacteria | Double cleanse + avoid high-silicone conditioner |
| D. Endocrine / Stress Type | Odor flares with menstrual cycle, exams, overtime | Androgens / cortisol | Diet + stress + sleep interventions |
| E. Self-Perceived but Not Confirmed by Others | Strong subjective odor, objectively normal skin | OlRS gray zone | See Section 7 (objective assessment first) |
In real life, archetypes often overlap — for instance, type B seborrhea plus type D stress at the same time. The integrated workup identifies the dominant driver first, then addresses the secondary contributors in order.
How do you run the 4-week home-care protocol for scalp odor?
Most scalp odor can start with a 4-week systematic home protocol: adjust wash frequency and technique, choose ingredients matched to your sebum and flora, and record odor and oiliness at weeks 0/2/4 — use a measurable flow to watch improvement, then decide whether medical intervention is needed.Before stepping into medical intervention, most scalp odor cases benefit from observing 4 weeks of structured home care. Please record at weeks 0 / 2 / 4:
- Odor intensity (self-rated, 0–10)
- Accompanying symptoms (flakes, itch, shine, erythema)
- Triggers (exercise / stress / hats / diet)
Week 0: Baseline + Product Audit
- List every shampoo, conditioner, and styling product currently in rotation, including ingredients (to surface possible residues and allergens)
- Photograph the scalp shine zone (phone with fill light, fixed angle)
- Self-rate odor intensity and log which times of day are worst
Weeks 1–2: Personalize Wash Frequency and Actives
Wash frequency principles:| Scalp type | Recommended frequency | Note |
|---|---|---|
| Oily (greasy by midday) | Once daily | Don't drop to every other day hoping to "reduce secretion" — it rebounds |
| Normal / combination | Every 1–2 days | Add a wash on heavy sweat or exercise days |
| Dry (prone to flakes) | Every 2–3 days | Avoid hot water + harsh degreasing shampoo |
- Antifungal route (Malassezia-dominant): Zinc Pyrithione 1–2% → Ketoconazole 1% → Selenium Sulfide 1% (rotate weekly; leave on 3–5 minutes)
- Keratolytic route (heavy flakes): Salicylic Acid 2–3%, 1–2 times per week
- Antibacterial route (bacterial-dominant): Piroctone Olamine, tea-tree-containing products (watch for allergy)
Week 3: Diet and Lifestyle Adjustments
- Reduce: high-fat foods (fried, butter-rich pastries), refined sugars (sweet drinks, desserts), alcohol
- Add: Omega-3 (deep-sea fish, flaxseed oil), zinc (oysters, nuts), B-complex (whole grains)
- Sleep: 7+ hours, consistent timing; sleep deprivation amplifies cortisol
- Stress management: 10–15 minutes of daily aerobic exercise, meditation, deep breathing (anything that lets you "downshift")
Week 4: Reassess and Decide Next Step
| Improvement | Next step |
|---|---|
| ≥ 70% improvement | Maintain current plan; transition to a stable maintenance rhythm (see Section 9) |
| 30–70% improvement | Fine-tune active combination, observe 2 more weeks |
| < 30% improvement | Schedule an Integrated Odor Clinic evaluation; consider Tier 1 prescription |
| No improvement + hair loss / severe redness | See a clinician immediately; differential diagnosis may be needed |
After home care doesn't work, what are the medical intervention tiers?
Medical intervention starts only after 4 weeks of home care show no change, on a "minimum necessary strength, re-evaluate at follow-up" principle: Tier 1 prescription topical antifungal/antibacterial washes, Tier 2 stronger or oral, Tier 3 stubborn or combined issues — stepping up one tier at a time, not maxing out from the start.If 4 weeks of home care don't move the needle, escalate to medical intervention. The principle is "lowest necessary intensity, with scheduled reassessment."
Tier 1: Prescription-Strength Shampoo
| Active | Indication | Use rhythm |
|---|---|---|
| Ketoconazole 2% (Rx) | Malassezia-dominant; OTC 1% ineffective | 2–3× per week, leave on 5 minutes |
| Ciclopirox 1% | Ketoconazole allergy or tolerance | Same as above |
| High-concentration Selenium Sulfide | Severe seborrhea | 2× per week, leave on 3–5 minutes |
Tier 2: Short-Term Topical Therapy
Targeted at the acute flare of seborrheic dermatitis with "odor + marked erythema / itch / scaling":
- Low-potency topical steroid (e.g., Hydrocortisone 1%), short course: 1–2× daily, no more than 2 weeks
- Topical calcineurin inhibitors (Tacrolimus, Pimecrolimus): for sensitive skin or patients unsuitable for long-term steroids
- Continue Tier 1 shampoo in parallel
Tier 3: Advanced Workup and Therapy
When Tier 1 + Tier 2 over 8 weeks fail to deliver improvement or symptoms keep relapsing:
- Microbiome testing (microbiota profiling): quantify Malassezia and bacterial composition
- Sebum analysis: lipidomic profiling to localize compositional abnormalities
- Oral antifungals (Fluconazole, Itraconazole): short courses for severe refractory cases; requires liver function monitoring
- Laser / red-light therapy: modulate sebaceous gland activity, typically 4–6 sessions
- Rare differentials: tinea capitis, follicular keratosis, rare metabolic disorders producing odor
Why don't we recommend applying underarm sweat-gland surgery to the scalp?
Short answer: it doesn't apply, and the risk far outweighs the benefit — scalp odor is driven by sebum and flora, not apocrine glands, and the scalp is dense with vessels, nerves, and follicles; forcing underarm sweat-gland surgery onto it neither fixes the root cause nor avoids harming follicles and blood supply.This is one of the most-asked questions in clinic, especially from patients who've seen successful axillary bromhidrosis surgery. The short answer: it doesn't apply, and the risk far outweighs the benefit.
Three Core Reasons
1. Wrong-mechanism mappingAxillary bromhidrosis procedures (rotational curettage, laser, miraDry) remove or ablate apocrine glands. Apocrine density on the scalp is extremely low, concentrated mostly behind the ears. The main driver of scalp odor is the sebaceous glands — but excising those is not clinically feasible (see reason 2).
2. Anatomical riskThe scalp has properties that make this dangerous:
- Highly vascular: capillary density per cm² far exceeds the axilla; intraoperative hemostasis is difficult
- Dense follicles: 100–200 follicles per cm² — surgically removing sebaceous glands almost inevitably damages follicles → permanent alopecia
- Visible scarring on the scalp: axillary scars hide in skin folds and hair; scalp scars can only be covered by long hair
On PubMed / Google Scholar, clinical studies on "scalp odor surgery" or "scalp apocrine gland excision" are sparse with small sample sizes. Major international dermatology guidelines (AAD, EADV) do not list surgery as a standard treatment for scalp odor.
The Rare Exception
The one situation that might warrant consideration: imaging or biopsy clearly confirming an abnormal apocrine distribution in a specific scalp region (e.g., certain hereditary apocrine ectopia), with that region serving as the primary odor source. In 20 years of clinic, the cases I've seen could be counted on one hand.
The Integrated Odor Clinic position is clear: scalp odor is solved by management, not by excision. Misapplying axillary surgical experience to the scalp is using the right tool on the wrong problem.
"I think I smell terrible, but everyone says they can't" — what's going on?
This may be Olfactory Reference Syndrome (OlRS): a small group strongly feel they smell, yet objectively family and friends notice nothing and exams find no source — here hunting for an "even stronger shampoo or treatment" won't help; what's needed is a different kind of evaluation and support.A small subset of patients say: "I think I smell terrible, but my family and friends say they don't notice anything." This is the gray zone of Olfactory Reference Syndrome (ORS / OlRS).
Why This Deserves Special Handling
Labeling it as "purely psychogenic, you're imagining it" causes two harms:
- A real, physiological microbiome imbalance gets overlooked (a strong subjective complaint with mild objective findings is genuinely possible)
- A stigmatized patient becomes even less likely to seek help
The Integrated Odor Clinic pathway:
Step 1 — Objective evaluation to rule out physiological factors- Full microbiome workup (microbiota, lipid profile)
- Dermatologic differential (seborrhea, folliculitis, other skin conditions)
- Third-party olfactory assessment (family member + medical staff, double-blind confirmation)
- Do not deliver a "psychogenic" conclusion; instead explain that "the physiological evaluation is normal, and subjective anxiety may have other contributors"
- Recommend a psychosomatic medicine or psychiatry evaluation (especially when accompanied by social avoidance or compulsive checking behaviors)
- In DSM-5, ORS is classified within the OCD spectrum and has dedicated therapies (CBT, SSRIs)
Even when objective findings are normal, the 4-week home-care plan has almost no downside and may improve subjective experience — more useful to the patient than a flat refusal of treatment.
Once the Phase 4 integrated assessment workflow is live, OlRS screening will be built into the initial visit. For now, you can self-assess at /assessment and then decide whether to consult further.
When should you visit the integrated clinic instead of trying another shampoo?
When 4 weeks of home care show no improvement, when there's scalp redness, oozing, or noticeable hair loss, when odor affects your social life, or when you're unsure which type you are — it's time to book an integrated evaluation rather than trying one shampoo after another.If any of the following hold, schedule an integrated evaluation rather than trying yet another shampoo:
- Less than 30% improvement after 4 weeks of structured home care
- Accompanying hair loss, scalp redness, marked dandruff, or itching
- Odor affecting social life, work, intimate relationships, or self-esteem
- Strong subjective odor not perceived by family or close friends (OlRS evaluation needed)
- Simultaneous odor in other regions (underarm, groin, feet) that needs integrated handling
The initial-visit workflow at the Integrated Odor Clinic (after Phase 2 goes live; for now, a standard dermatology consultation can be scheduled):
- History (10–15 min): odor history, family history, lifestyle, medications, current product audit
- Objective examination (10 min): dermoscopy, distribution of oily zones, dandruff grading
- Odor evaluation (5 min): clinician-side olfactory assessment, with a third-party companion when needed
- Optional microbiome assessment (10 min): sebum sampling sent for microbiota analysis
- Integrated plan (5–10 min): a personalized Tier 0–3 pathway based on the evaluation
After it improves, how do you maintain across 3/6/12 months without relapse?
Scalp odor is about "stable maintenance," not "one-time cure": after improvement, keep the most effective washing and ingredients as routine, re-evaluate at 3 months, fine-tune at 6, and confirm stability at 12 — a maintenance rhythm prevents relapse better than a one-off sprint.Integrated odor management is about stable maintenance, not "one-time cure." Recommended long-term rhythm:
3-Month Checkpoint
- Self-rated odor intensity compared with baseline
- Prescription medication use: can the frequency step down? (e.g., from Ketoconazole 3×/week to 1×/week)
- Lifestyle factors review: have diet, sleep, and stress drifted back to old habits?
6-Month Checkpoint
- Repeat microbiome assessment (if Tier 3 was used)
- Seasonal adjustment: summer requires more frequent cleansing for sweat; winter requires careful moisture balance
- Re-evaluate whether odor is appearing elsewhere on the body (integrated view)
12-Month Checkpoint
- Annual review: which months worsened, and what life events correlated
- Fine-tune the long-term maintenance plan: is a "minimum maintenance dose" mode now feasible?
- Overall health check: any changes in hormones, metabolism, or nutrition
FAQ — 12 of the Most Common Clinic Questions
Q1. Is scalp odor "apocrine bromhidrosis" spreading up to the scalp?
Only in very rare cases. Apocrine density on the scalp is low (concentrated behind the ears). The vast majority of scalp odor is the interaction of sebaceous glands, bacteria, and Malassezia yeasts — not the apocrine bromhidrosis pattern you see in the underarm. A small number of people with more developed retroauricular apocrine glands may notice a localized odor there, but that's a regional phenomenon distinct from the overall greasy scalp odor mechanism.
Q2. Can I treat scalp odor using the same surgery as axillary bromhidrosis?
Not recommended. International literature support is very limited, and the scalp is highly vascular and densely follicular — surgical removal of sebaceous glands carries risk far exceeding benefit and can cause permanent alopecia. This clinic does not advocate transferring apocrine surgery from the axilla / areola / groin to the scalp. We only discuss it in the rare scenario where imaging or biopsy clearly confirms an abnormal apocrine distribution.
Q3. I've used anti-dandruff shampoo and there's still odor — am I using it wrong?
Possibly, for several reasons: (1) insufficient active concentration (most OTC products are 0.5–1%; prescription-grade Ketoconazole is 2%); (2) leave-on time too short (3–5 minutes is recommended); (3) the odor source isn't Malassezia but other bacteria or product residue; (4) coexisting seborrheic dermatitis needs short-term topical therapy. If 4 weeks of home care don't produce improvement, come in for reassessment.
Q4. Does diet really affect scalp odor?
It has an indirect effect. High-fat foods, refined sugars, and alcohol amplify sebaceous secretion and provide more fuel for bacteria and yeasts; deficiency of Omega-3 and zinc can affect sebum composition; severe dehydration concentrates sweat and sebum. Dietary adjustment is usually adjunctive rather than primary, and effects emerge gradually over 4–8 weeks.
Q5. Is scalp odor related to stress?
Yes. Cortisol (the stress hormone) amplifies androgen-driven stimulation of sebaceous glands, and stress itself alters apocrine activity (e.g., behind the ears). Many people notice scalp odor worsens during high-pressure work periods, before exams, or with sleep deprivation — this is a real physiological mechanism, not psychological misperception.
Q6. I think I smell bad but my family says I don't. What do I do?
This may fall into the "Olfactory Reference Syndrome (OlRS)" gray zone — a large gap between subjective odor intensity and objective findings. The clinic does not deliver a "psychogenic" verdict outright. We first run an objective microbiome workup to rule out physiological factors. If the full objective panel is normal but subjective anxiety persists, we recommend pairing with a psychosomatic medicine evaluation (this will be more systematic in the Phase 4 integrated workflow).
Q7. Can scalp odor be "cured"?
We don't use absolute language like "cure" — sebaceous glands and the microbiome are dynamically regulated, and the goal is to reduce odor to a level that doesn't bother you or those around you and to maintain it stably. Most people significantly reduce odor within 4–12 weeks on a structured plan, but sustained maintenance is required (e.g., wash frequency, antifungal rotation). Individual results may vary.
Q8. What's the difference between prescription-grade Ketoconazole and OTC versions?
OTC products (e.g., Nizoral) contain 1% Ketoconazole; prescription-grade is 2%. The difference isn't only concentration — pharmaceutical-grade quality control and vehicle formulation give the prescription product better scalp penetration. For moderate-to-severe Malassezia overgrowth, the clinical improvement rate at prescription strength is meaningfully higher. For long-term use, discuss a rotation strategy with your physician to avoid single-active tolerance.
Q9. Can I use two antifungal shampoos at the same time?
You can — but rotation, not stacking, is the rational approach. For example: Mon/Wed/Fri Ketoconazole, Tue/Thu/Sat Zinc Pyrithione, Sunday a gentle regular shampoo. Rotation reduces single-active tolerance risk. Stacking two antifungal actives in the same wash doesn't boost efficacy but does increase irritation risk.
Q10. Is scalp odor contagious to family members?
Not in the "infectious disease" sense. The microbiome is individual — every scalp's microbiota is different. But shared towels, pillowcases, and combs can transfer some microbes, especially during active seborrheic dermatitis flares. Recommendations: weekly pillowcase washing, individual towels, no shared styling tools.
Q11. Do hats and helmets make scalp odor worse?
Yes. Prolonged hot, sealed environments: (1) promote sebum secretion; (2) create a moist environment for bacterial and fungal proliferation; (3) physically press product residue into pores. Suggestions: allow the scalp 5–10 minutes of airflow every 1–2 hours, rotate or air-dry helmet liners regularly, wash hair as soon as possible after exercise.
Q12. When will the "Odor Map Initial Consultation" launch?
Planned for Phase 2 (June–July 2026), as a dedicated 30–45 minute integrated initial visit covering six stations — scalp, oral, body odor, intimate, metabolic — plus optional microbiome testing. For now you can schedule a standard dermatology consultation to understand your situation.
Related Reading
- Scalp Odor: Antifungal or Antibacterial Shampoo? 5 Signs
- Wash Hair Daily or Every Other Day? Scalp Microbiome
- Oily Smell on Your Pillow After 40? Middle-Aged Scalp Odor
- Stale Smell on Your Pillow After 40? 2-Nonenal Explained
- Bromhidrosis Guide: Causes, Diagnosis, Treatment & Recovery
- Scalp Odor Integrated Assessment
- Midlife Body Odor & Aging Odor Guide
A Closing Note
Scalp odor is something many people quietly endure but rarely discuss systematically. The root cause isn't "find the right shampoo" as a single-point fix — it lies in understanding the dynamic nature of the microbiome and building a feedback loop of "assess → intervene → maintain → reassess."
The core position of the Integrated Odor Clinic: odor is a signal, not a defect. It tells you something is out of balance between your body and its microbes — possibly from diet, stress, medication, skin-barrier changes, or several factors stacked together. Reading the signal matters more than masking it.
Related Reading
- Scalp Odor: Antifungal or Antibacterial Shampoo? 5 Signs
- Wash Hair Daily or Every Other Day? Scalp Microbiome
- Bromhidrosis Guide: Causes, Diagnosis, Treatment & Recovery
- Scalp Odor Integrated Assessment
If this guide gives you a clearer sense of your own scalp odor, you're welcome to use the decision tree in Section 8 and decide whether to book an integrated evaluation. If you're still in the middle of the 4-week home-care plan, please record the changes at weeks 0 / 2 / 4 carefully — that record is the most useful data point during a clinic evaluation.