
Why Another Bromhidrosis Guide?
Most people first notice their body odor in adolescence — and most never get a clear framework for understanding what's actually happening or what the realistic options are.
In 20 years of clinical practice, the single most common pattern I see in the consultation room is not severity — it's uncertainty. Patients don't know which grade they fall into, don't know whether to try conservative treatment or move straight to surgery, don't know whether axillary odor and areolar odor are the same problem.
This guide consolidates the questions I get asked most often into one path: causes → self-grading → treatment ladder → surgical options → recovery timeline → long-term follow-up. By the end you should be able to answer:
- Which severity grade fits my situation?
- Is the odor at different body regions (underarm, areola, perineal) handled the same way?
- Antiperspirant, Botox, micro rotational curettage — where should I start on the ladder?
- How long until I can return to normal life after surgery? What's the recurrence rate?
Individual outcomes vary. This guide provides a decision framework, not a diagnosis. The final treatment choice still requires in-person evaluation.
Multi-site odor? Start with the map, then the self-check. If you have odor in more than one area, see the Odor Map for site-by-site triage first, then run the Self-Assessment to score severity — usually faster than booking a single specialty up front.
What is bromhidrosis, and is the cause really not "poor hygiene"?
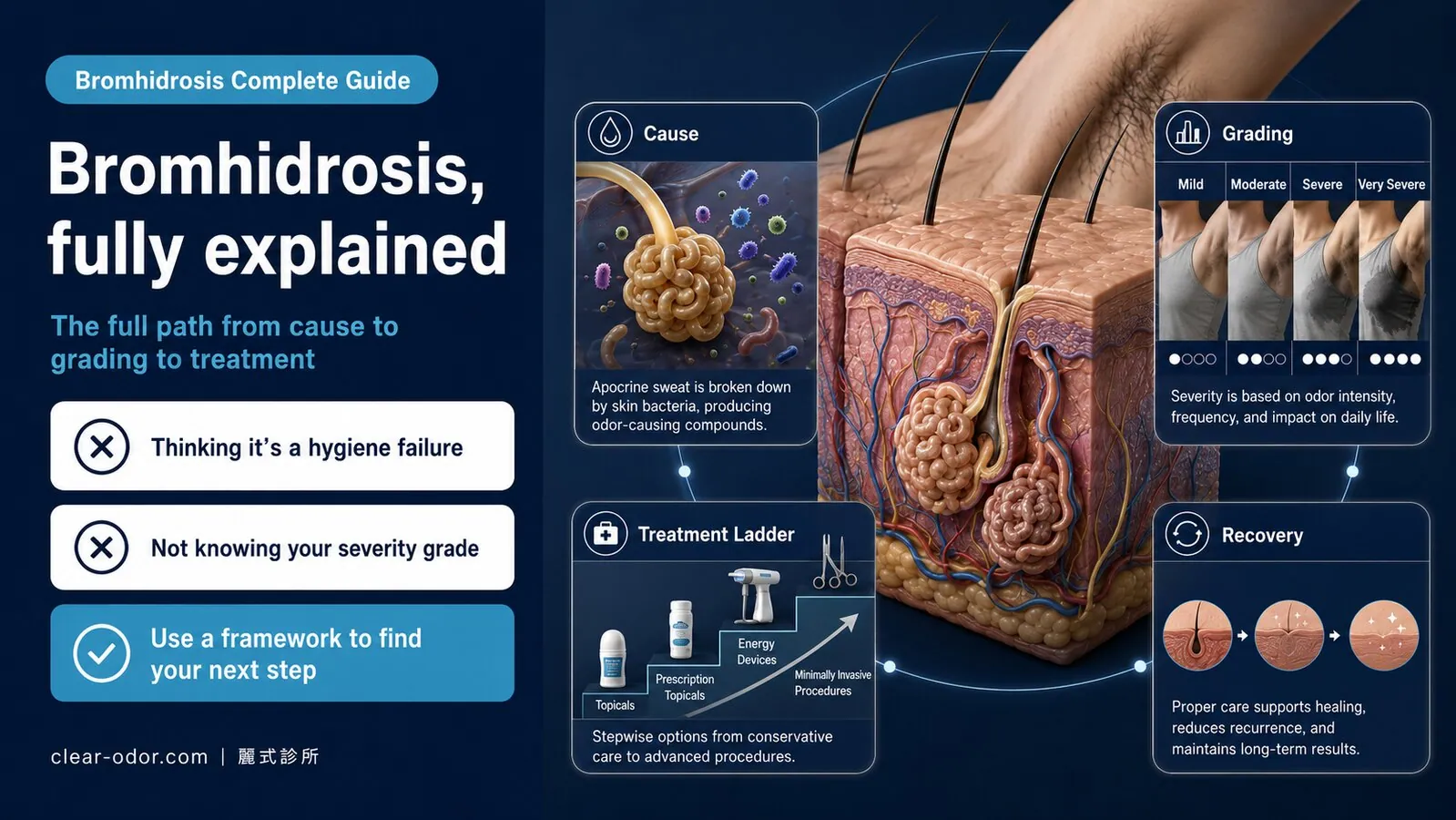
Bromhidrosis is the medical term for underarm odor; it arises when apocrine secretions are broken down by skin-surface bacteria into the characteristic smell — driven by genetics and hormones, not poor hygiene, which is why washing harder only suppresses it temporarily and can't cure it.Bromhidrosis is the medical term for the characteristic body odor most commonly associated with the underarms, but it also covers the areolae, perineum, and groin.
A frequent misconception: sweat itself smells. It does not. Fresh sweat is odorless. The smell comes from a three-part chemical reaction:
- Apocrine gland secretions — protein, fatty acids, steroid precursors
- Skin microflora — primarily Corynebacterium spp. and Staphylococcus spp.
- Enzymatic breakdown — bacteria cleave long-chain apocrine secretions into short-chain volatile fatty acids (such as 3-methyl-2-hexenoic acid and 3-hydroxy-3-methyl-hexanoic acid). These short-chain acids are the chemical signature of bromhidrosis.
In short: active apocrine glands + dense skin flora = readily produces odor. This is a constitutional issue, not a hygiene issue.
Why Is Bromhidrosis Genetic?
East Asian populations show a strong correlation between bromhidrosis and the ABCC11 gene (538G→A polymorphism). The A/A genotype produces thin, weakly odoriferous apocrine secretions; G/G and G/A genotypes produce typical bromhidrosis and correlate with wet earwax.
This is why I almost always ask in the clinic: "Is your earwax wet or dry?" Wet earwax is essentially a phenotypic marker of active apocrine glands.
When Do Apocrine Glands Become Active?
Apocrine glands are driven by sex hormones: they begin developing at puberty (ages 10–14), mature through the late teens, peak in activity between 20 and 40, and gradually atrophy after age 50 — though they never fully disappear.
That's why bromhidrosis typically appears in adolescence, peaks in midlife, and slowly diminishes with age — but does not "spontaneously resolve," because the underlying glandular tissue persists.
Will bromhidrosis go away on its own? Is surgery the only option?
Bromhidrosis does not resolve on its own — it is driven by your apocrine gland constitution, and once those glands have developed they keep secreting, so no amount of washing does more than temporarily mask it. But surgery is not the only option either: mild-to-moderate cases can first use antiperspirants and Botox to bring the odor down to an acceptable level, and only people who want long-term stability — without managing it again every few months — need to move toward gland-removal surgery.Many people hope that "it should settle once puberty is over" or "it will fade with age if I just put up with it." Physiologically, that is only half true. Apocrine glands are driven by sex hormones; they do atrophy gradually after age 50 and the odor may soften, but during your 20s to 40s — exactly when social life and appearance matter most — they are at their activity peak and do not recede on their own.
As for "is surgery the only option," the answer is no. Think of the choices as three tiers, stepping up with how much it bothers you:
- Temporary masking (antiperspirants, deodorant): effective for grade 1–2 mild cases, reverses as soon as you stop, and does nothing to the glands themselves.
- Temporary suppression (Botox): lasts 4–6 months, suited to short-term occasions or those still deciding, but needs repeating.
- Long-term clearance (micro rotational curettage surgery): treats the apocrine glands directly and is currently the most evidence-backed long-term option for moderate-to-severe bromhidrosis; our clinic aims for complete apocrine gland clearance, with no recurrence reported in clinical follow-up (individual results may vary).
In other words, "will it go away" and "should I have surgery" are two separate questions: the first answer is no, while the second depends on your severity, how thorough you want to be, and whether you are willing to repeat treatment every few months. If you are not sure which tier you fall into, when you book a one-on-one assessment we will first locate your severity and then walk through the options one by one — the consultation is not tied to any procedure.
Are bromhidrosis and hyperhidrosis the same problem?
No — bromhidrosis is an "odor" problem from apocrine glands plus bacteria, while hyperhidrosis is a "sweat volume" problem from eccrine glands; they often coexist and get confused, but their treatments differ (deodorizing vs reducing sweat), so sorting them out first prevents using the wrong approach."My underarm both smells and sweats a lot — are these the same problem?" This question comes up every week.
The answer: not the same problem, but commonly co-occurring. The difference comes down to two different sweat gland types:
| Comparison | Bromhidrosis | Hyperhidrosis |
|---|---|---|
| Gland source | Apocrine | Eccrine |
| Secretion | Viscous, contains protein + lipids | Watery, contains electrolytes |
| Distribution | Underarm, areolae, perineum, groin | Whole body (palms, soles, forehead, axillae focal) |
| Odor | Has characteristic odor | Odorless |
| Triggered by | Sex hormones, emotion | Heat, emotion, spicy food |
| Treatment goal | Reduce/remove apocrine glands | Block nerve signal to eccrine glands or destroy glands |
Four typical clinical patterns:
- Bromhidrosis alone — distinct odor, normal sweat volume → treatment targets apocrine glands
- Hyperhidrosis alone — high sweat volume, no odor → treatment targets eccrine glands (Botox, miraDry, in severe cases ETS)
- Combined bromhidrosis + hyperhidrosis (most common in clinic) — both gland types active → one surgery can address both (micro rotational curettage reduces both apocrine and eccrine glands simultaneously)
- Compensatory hyperhidrosis — heavy sweating on torso/back/legs after ETS sympathectomy → a separate problem with a different treatment pathway (see the deep-dive on compensatory hyperhidrosis)
How does bromhidrosis differ across the underarm, areola, perineum, and children?
All are odor problems in apocrine-rich regions, but each has different clinical considerations: the underarm is small enough to clear completely, the areola must preserve breastfeeding function, the perineum heals more slowly, and children depend on developmental timing — so treatment strategy varies by region.Many people don't realize "bromhidrosis" spans multiple body regions — fundamentally they're all the same problem (odor from apocrine-rich skin), but each region has distinct clinical considerations.
a. Axillary Bromhidrosis
The most common form. Underarm apocrine density is the highest on the body — about 30–40% of all apocrine glands sit in the axillae.
- Typical onset: post-puberty, peak 20–40
- Severity scale: 5-level odor-severity self-assessment (from no odor to detectable from > 1 m)
- Treatment ladder: antiperspirant → Botox (temporary) → micro rotational curettage (long-term)
- Detail page: Axillary bromhidrosis treatment
b. Areolar Bromhidrosis
The peri-areolar region also carries apocrine glands — fewer total than the axillae, but highly concentrated, which can make the localized odor more noticeable.
- Common demographic: women aged 30–50 most often present
- Special considerations: surgery must preserve lactation (avoid disrupting mammary duct architecture) and avoid permanent nipple sensitivity change
- Treatment ladder: conservative measures have limited effect → micro-surgical approach is the primary option
- Detail page: Areolar bromhidrosis treatment
c. Perineal Bromhidrosis
Apocrine odor at the perineum, groin, or peri-anal region — often misidentified as infection or hygiene failure. The underlying biology is identical to axillary bromhidrosis.
- Differential first: rule out bacterial vaginosis, candidiasis, and fistula before attributing odor to apocrine glands
- Treatment ladder: after infection is excluded, micro-surgical apocrine reduction is the main long-term option
- Detail page: Perineal odor treatment
d. Pediatric Bromhidrosis
Bromhidrosis appearing at 10–14 years old in early puberty — this age group carries the highest risk of social isolation and bullying, so I recommend active management rather than waiting it out.
- Surgical timing: apocrine glands are still maturing through puberty, so surgery is typically deferred to 14–16 years (after development stabilizes)
- Conservative bridge: antiperspirants and Botox can carry the patient through the interim
- Detail page: Pediatric bromhidrosis treatment
Which severity grade is your bromhidrosis, and how do you self-grade?
We use a simple 5-level odor-severity self-assessment: from barely detectable, to noticeable only up close, to obvious the moment you enter a room — checking yourself against this scale is the first step to deciding whether conservative measures or surgery fit.Use this 5-level odor-severity self-assessment:
| Grade | Description | Recommended action |
|---|---|---|
| 0 | No odor — undetectable to self and others | No intervention needed |
| 1 | Detectable on close inspection — mild after exercise/stress | Hygiene + antiperspirant suffice |
| 2 | Detectable at close range (< 30 cm) | Antiperspirant primary; Botox optional |
| 3 | Detectable at normal social distance (30 cm – 1 m) | Active treatment recommended — Botox (temporary) or surgery (long-term) |
| 4 | Detectable from > 1 m | Surgery strongly recommended — conservative measures have limited yield |
Common Self-Assessment Pitfalls
- Olfactory adaptation: people habituate to their own scent — "I don't smell anything, but others do" is real. Have a trusted family member help calibrate.
- Temporal variation: odor fluctuates with exercise, emotion, menstrual cycle, and diet. Judge the weekly average rather than any single moment.
- Subjective distress: some patients with grade 1 odor experience severe social anxiety. Subjective burden should weigh alongside objective grading in the treatment decision.
What treatment options exist, and how do you step up the ladder?
Treatment should climb a ladder, not jump straight to surgery: from conservative measures like antiperspirants and deodorants, to botulinum toxin, to minimally invasive surgery; pushing the lower-invasiveness options to their ceiling first and stepping up only if needed is the most rational order.Bromhidrosis treatment should not "jump straight to surgery." There's a rational ladder — escalate based on effectiveness and cost.
Rung 1: Daily Care and Antiperspirants (Suitable for Grades 1–2)
- Regular cleansing — wash underarms 1–2× daily with neutral soap
- Hair trimming — reduces surface area for bacterial colonization
- Aluminum-chloride antiperspirants (Driclor, ClinicalStrength) — mechanism is sweat duct occlusion; apply at bedtime, rinse on waking
- Antimicrobial body wash (triclosan or chlorhexidine)
⚠️ Limitations: no direct effect on apocrine glands; effect ceases when use stops; insufficient for grade 3–4.
Rung 2: Botox Injection (Suitable for Grades 2–3, Surgery-Averse)
Botox blocks the acetylcholine signal between sympathetic nerves and sweat glands — clear effect on hyperhidrosis and indirect suppression of apocrine activity.
- Single-session duration: 4–6 months
- Per-session cost: USD 800–1,500 (Taiwan) for bilateral axillae
- Long-term cost: 2 sessions per year × 3 years ≈ USD 5,000–9,000 — often more expensive than one-time surgery over the long run
- Best fit: short-term need (wedding, interview, exam), surgical contraindication, or trying it before committing to surgery
Rung 3: Microwave / Radiofrequency (e.g., miraDry)
- Mechanism: microwave energy destroys superficial sweat glands (both apocrine and eccrine)
- Per-session cost: USD 2,300–4,000
- Durability: 70–90% of patients maintain effect at 1 year; some report odor return at 2–3 years
- Limitation: energy delivery is blind (cannot see the gland) and uniformity depends on skin thickness — deeper apocrine glands may not be fully ablated. This is why miraDry is best suited to mild-moderate (grade 2–3) cases.
Rung 4: Micro Rotational Curettage Surgery (Suitable for Grades 3–4, Long-Term Stability)
This is our core technique and the best-evidenced long-term option for moderate-to-severe bromhidrosis.
Mechanism: A 5–7 mm micro-incision is made in the axilla. A rotational curette is inserted to directly visualize and remove the apocrine glands and most eccrine glands at the sub-dermal layer. Characteristics:- 5–7 mm incision (not a large open excision)
- Direct visualization — glands are physically seen and removed (unlike microwave's blind destruction)
- Simultaneously reduces apocrine (odor) + eccrine (sweat) glands — one surgery addresses both
- Local anesthesia, outpatient, same-day discharge
- Stable long-term — < 5% recurrence at 5-year follow-up
Full surgical detail, comparison with other techniques, indications, and contraindications: Axillary bromhidrosis surgical treatment.
Which treatment should you actually choose?
There's no single answer — decide based on severity, how thorough an effect you want, the invasiveness and recovery you'll accept, and your life needs; the same person's answer can change over time, and the point is to pick the option that best fits your weighting, not the most powerful one."Which treatment should I choose?" — there's no single answer. Decide based on these five dimensions:
Dimension 1: Severity
- Grade 1–2: start with conservative measures (hygiene, antiperspirant) — usually sufficient
- Grade 2–3: conservative + Botox combination
- Grade 3–4: surgery is the primary option — conservative has limited effect; repeated Botox costs more long-term
Dimension 2: Timeline
- Short-term (event within 6 months): Botox (effect in 4 weeks, lasts through event)
- Long-term (permanent solution): surgery
Dimension 3: Cost
- Botox every 4–6 months × USD 800–1,500 — 3-year total ≈ USD 5,000–9,000
- Micro rotational curettage one-time USD 4,000–6,000 (Taiwan) — 3-year horizon: surgery is the more economical choice
Dimension 4: Surgical Tolerance
- Can accept local anesthesia + 7-day recovery: surgery is viable
- Cannot accept any surgery or downtime: Botox or miraDry
Dimension 5: Combined Hyperhidrosis?
- Bromhidrosis alone: surgery or miraDry
- Hyperhidrosis alone (no odor): Botox, miraDry, or — in severe refractory cases — ETS (with the caveat that ETS carries 50–70% risk of compensatory hyperhidrosis)
- Combined: micro rotational curettage addresses both in one operation
Once you decide on surgery, what do you prepare in the 2 weeks before?
The 2-week pre-op window directly shapes recovery quality: avoid factors that increase bleeding, adjust any medications that need pausing (with your doctor), stop smoking, and arrange time off and a ride home — good preparation means smoother recovery and fewer complications.If you decide on micro rotational curettage, the 2-week pre-op window directly affects recovery quality.
14 Days Pre-Op
- Stop anticoagulants (aspirin, Plavix) — only after consulting the prescribing physician
- Stop fish oil, ginkgo, ginseng, vitamin E, and other supplements that may affect coagulation
- Increase protein and vitamin C intake (supports wound healing)
3 Days Pre-Op
- No alcohol, no spicy food
- Avoid heavy weight training (axillary muscle soreness can complicate post-op movement)
1 Day Pre-Op
- Shave underarm hair (not too close to surgery time — fresh follicle microtrauma raises infection risk)
- Prepare 5 loose-fitting button-down shirts (for the 7-day compression dressing period)
- Arrange schedule flexibility for the next 7 days (no sick leave needed, but ability to modulate activity helps)
After bromhidrosis surgery, how soon can you return to normal life?
A typical timeline: the first 7 days are most uncomfortable and compression matters most, showering at Day 7, most back to work by Day 14, most exercise by Day 30, and Day 90–180 for final-result evaluation and scar maturation — looking "healed" on the surface doesn't mean tissue remodeling is complete.Most patients want to know "when can I return to normal life?" Here's the typical timeline:
Day 0 (Surgery Day)
- Local anesthesia, surgery time ~60–90 minutes
- Compression dressing applied immediately, same-day discharge
- 2–4 hours after anesthesia wears off there is a deep ache, controllable with oral analgesics
Days 1–3
- Compression dressing must remain in place — do not remove on your own
- Ice pack ≥ 3× per day, 20 minutes each
- Limit upper-body large movements (no lifting heavy objects, no overhead cleaning)
- Most patients return to office work; avoid strenuous activity
Day 7
- Follow-up visit to remove dressing and inspect the wound
- The 5–7 mm incision is closed and healing — showering permitted
- Begin light upper-body movement; still avoid exercise
Day 14
- Sutures removed (or absorbable sutures complete dissolution)
- Resume general activities; still avoid weight training and swimming
Day 30
- Most swelling resolves; odor improvement clearly noticeable
- All routine exercise can resume
Month 3
- Scar transitions from pink to pale; tissue remodels
- Odor and sweat improvement stabilize
Month 6
- Scar matures (the 5–7 mm incision in the axillary fold is nearly invisible)
- Long-term outcome assessment endpoint
What are the long-term results and recurrence rate of the surgery?
Micro rotational curettage clears roughly 85–95%, and most patients maintain good results long-term; a minority have residual odor because apocrine glands aren't neatly arranged or because skin blood supply must be preserved, and this can be touched up within a year — a reasonable balance between safety and thoroughness.Five-year follow-up of patients undergoing micro rotational curettage —
- 5-year recurrence rate (odor returning to ≥ grade 3): < 5%
- Satisfaction: > 90% of patients say they "would do it again"
- Common causes of residual odor:
- Significant weight gain altering skin tension and prompting regrowth of residual glands
- Certain medications (some antipsychotics) affecting sweat gland output
- Patients with extreme severity (grade 5) — a small number need a secondary touch-up
Individual outcomes vary. During pre-op evaluation we clearly communicate the expected improvement range and possible limitations.
Frequently Asked Questions (FAQ)
Q1: Will surgery leave a scar?
The 5–7 mm incision sits in the natural axillary fold. At 6 months it is usually nearly invisible — most patients can't find it on photographs.
Q2: Will surgery damage nerves?
Direct visualization allows us to avoid the major axillary neurovascular structures (axillary nerve, long thoracic nerve). Rare transient arm numbness typically resolves within 4–8 weeks.
Q3: Can underarm bromhidrosis and palmar hyperhidrosis be treated in the same surgery?
Different regions require different approaches. Axillary bromhidrosis uses micro rotational curettage; palmar hyperhidrosis is primarily treated with ETS sympathectomy, which carries a 50–70% risk of compensatory hyperhidrosis. The trade-offs need to be discussed thoroughly. See palmar hyperhidrosis treatment.
Q4: How long does a Botox injection last?
A single axillary injection lasts 4–6 months and must be repeated. Long-term cumulative cost typically exceeds that of one-time surgery.
Q5: Do antiperspirants cause breast cancer?
There is no scientific evidence supporting a link between aluminum-salt antiperspirants and breast cancer. Multiple large studies (e.g., 2004 NCI review) have failed to find any correlation.
Q6: Can adolescents under 14 have surgery?
Apocrine glands are still maturing during early adolescence, so surgery is generally deferred until 14–16 years when development stabilizes. Antiperspirants and Botox bridge the interim.
Q7: Will bromhidrosis recur after surgery?
5-year recurrence rate < 5%. The small minority who recur are usually extremely severe initial cases or have undergone significant weight changes.
Q8: Can I breastfeed after surgery? (For areolar bromhidrosis)
The micro-surgical technique does not transect mammary ducts, and most patients retain full breastfeeding function. That said, completing breastfeeding before surgery is the most conservative approach.
Q9: I have a keloid tendency — can I still have surgery?
Keloid-prone patients require careful evaluation. The axillary fold incision typically heals well in most keloid patients, but we discuss a prophylactic intralesional steroid plan pre-op.
Q10: What if the outcome falls short of expectations?
A small number of patients with residual odor at 6-month evaluation can undergo a touch-up procedure. If needed, necessary revisions can be arranged within 1 year.
When should you book a consultation?
When conservative measures are maxed out and it still bothers you, when odor affects your social life or confidence, when you want to understand your severity and full options, or when you're unsure whether it's odor or sweating — it's worth an in-person evaluation to match a plan to your situation.If any of the following apply, an in-person evaluation is worthwhile:
- Odor reaches grade 3 or above (detectable at social distance)
- Antiperspirants used ≥ 6 months without sufficient effect
- Considered Botox but tired of the long-term cost and repeat injections
- Combined bromhidrosis + hyperhidrosis — want to address both at once
- Adolescent in your family with bromhidrosis affecting social confidence
The evaluation covers: detailed history (family history, symptom timeline, prior treatments), objective grading, apocrine distribution palpation, and a discussion of the treatment pathway that best fits your situation.
The evaluation fee is not tied to subsequent treatment — a consult-only visit with no surgery commitment is fine.
Closing: Returning the Decision to You
Bromhidrosis is not "poor hygiene" and it's not "hopeless." It has a clear etiology, a complete treatment ladder, and a real choice to make based on your severity and life context.
The goal of this guide is not to push you toward surgery — it's to give you an accurate framework for assessing your situation so you know which direction to step next.
If anything remains unclear after reading, you're welcome to book a one-on-one evaluation. In the clinic we walk through each option side by side.
Related Reading
- Underarm Odor: Antiperspirant vs Botox vs Surgery
- How Long Is Underarm Odor Surgery Recovery? Aftercare Guide
- Areola Odor Surgery: Will It Affect Breastfeeding?
- Hyperhidrosis vs Compensatory Sweating: Before ETS Surgery
- Child Teased for Body Odor at School? A 5-Step Parent Guide
- Bad Breath Brushing Won't Fix? 5 Sources & Which Doctor
- Foot Odor Won't Wash Off? Causes & a 4-Week Home Protocol
- Whole-Body Metabolic Odor: TMAU, Diabetes & Liver Signals
- Aging Body Odor vs Bromhidrosis: 3 Smells, How to Tell
- Axillary Bromhidrosis
- Areola Bromhidrosis
- Perineal Bromhidrosis
- Pediatric Bromhidrosis
- Hyperhidrosis & Compensatory Sweating
- Palmar Hyperhidrosis
- Oral / Halitosis Integrated Triage
- Foot Odor Integrated Assessment
- Systemic / Metabolic Odor Screening
- Midlife Body Odor & Aging Odor Guide
- Body Odor & Hyperhidrosis Conditions