Why we wrote this guide
Every week, we hear variations of the same questions in clinic:
- "I brush every day, use mouthwash, and get my teeth cleaned regularly — but a coworker still mentioned my breath. Am I brushing wrong?"
- "My dentist says my teeth are fine, but I can smell something the moment I open my mouth. Where is the problem really coming from?"
- "I thought tonsil stones would be solved once I squeezed them out — why do they keep coming back?"
- "My family says I have bad breath, but I don't smell anything after I brush. Is something wrong with my sense of smell?"
Behind these questions is the same underlying misconception: the assumption that breath odor has a single source, and that finding the right tool (the right brushing technique, the right cleaning, the right food) will solve it.
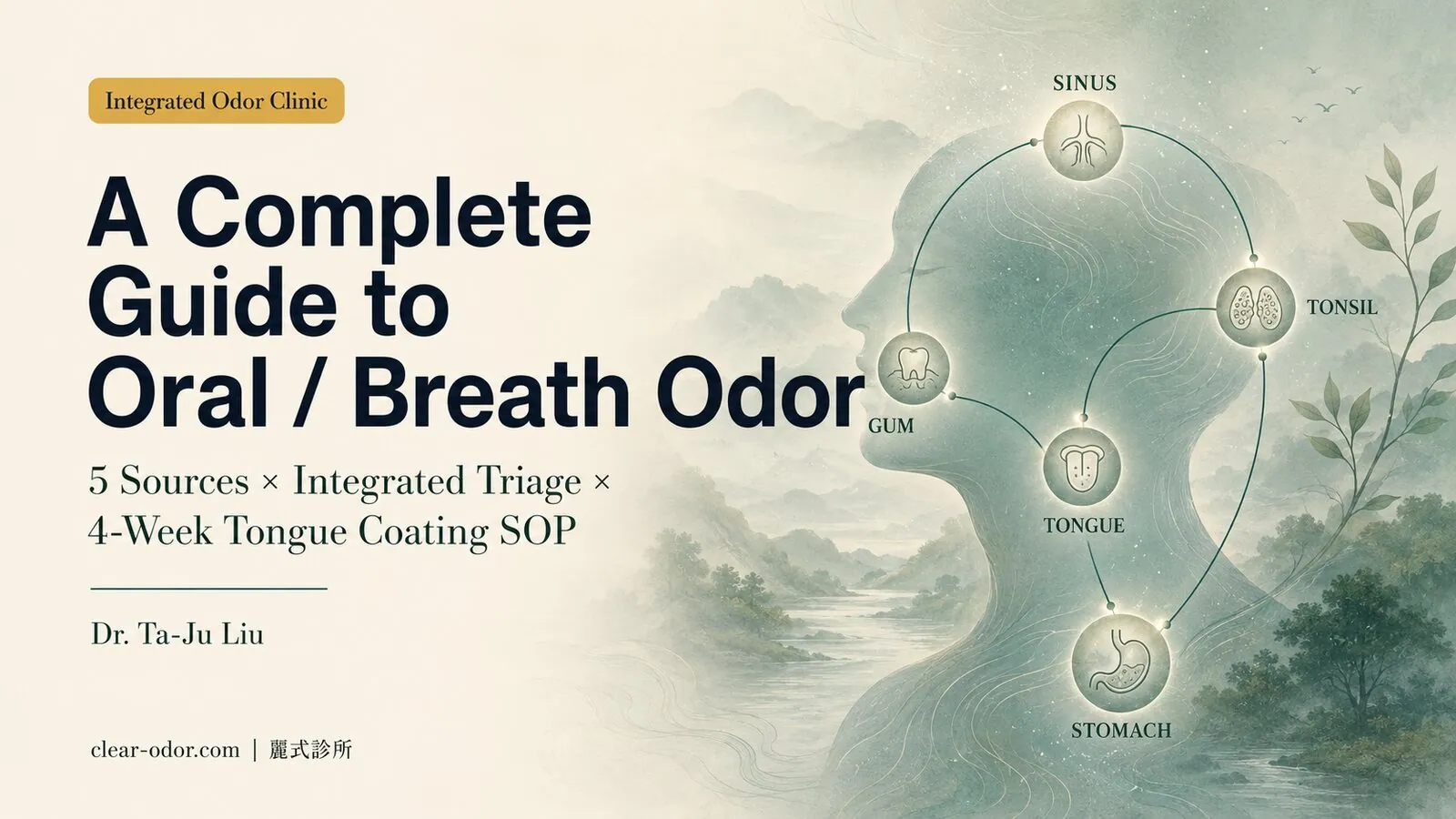
In reality, breath odor has at least 5 broad sources — tongue coating, periodontal disease, tonsil stones, post-nasal drip, and GERD. Each has a different mechanism, each requires a different specialty, and they very often coexist. Roughly 30-40% of patients with long-standing bad breath have a "primary source + 1-2 secondary sources" pattern, and bouncing between single specialties (purely dental or purely ENT) tends to keep missing the dominant cause.
The role of the Integrated Odor Clinic is not to "treat everything ourselves," but to do an Integrated Triage first, identify the dominant source, and then map out an individualized referral path — so you stop cycling between doctors and surface-level treatments.
This guide distills the most-asked decision criteria from 20 years of clinic work, and provides a reading framework that lets you see which subtype you most likely belong to, and where to start, before you ever sit down for a consultation. After reading, you should be able to answer:
- Which dominant source is driving my breath odor?
- When should I start with an Integrated Triage, and when can I go straight to a single specialty?
- How do I run a 4-week home tongue-coating management plan, and when do I need to escalate to a prescription?
- Why do tonsil stones keep coming back after squeezing, and what's the root-level solution?
- "I smell it strongly but others don't" — what do I do in that situation?
Individual results may vary — this guide provides a framework for thinking, not a diagnostic conclusion. The actual treatment path still needs to be decided in person after a face-to-face evaluation.
Multi-site odor? If you have odor in more than one area, see the Odor Map for site-by-site triage first to identify the primary source before diving into this guide.
How do breath odor and body odor differ mechanistically?
Breath odor isn't "B.O. in the mouth" — body odor comes from apocrine glands, while breath odor mainly comes from bacterial metabolism in the mouth (tongue coating, gums) and, less often, sinus or GI sources; different mechanisms, so treating breath odor as body odor sends you down the wrong path.Many people read online articles and assume breath odor is "the same thing as body odor" — a misconception that often leads to the wrong treatment path.
1. Body odor (axillary / areolar / perineal)
The main driver is the apocrine glands, which secrete proteins and lipids that are metabolized by specific bacteria (such as Corynebacterium) into short-chain fatty acids and thiol compounds. Characteristics:
- Only appears from puberty onward
- Localized to specific regions (underarms, areola, perineum, ear canal)
- Physically removing the apocrine glands can substantially reduce it (which is why surgery works)
2. Breath odor (driven by 5 main sources)
There are virtually no apocrine glands inside the oral cavity, and the chemical sources of odor are different — primarily volatile sulfur compounds (VSCs), short-chain fatty acids, and volatile amines. There are at least 5 sites where these gases are produced:
- Tongue coating: anaerobic bacteria on the posterior third of the tongue break down food debris and shed epithelial cells, producing hydrogen sulfide and methyl mercaptan (the most common source, accounting for roughly 60-70%)
- Periodontal pockets / caries: chronic inflammation within deep bacterial biofilms, plus protein breakdown
- Tonsillar crypts: accumulation of calcified food debris, shed epithelial cells, and bacteria (tonsil stones)
- Post-nasal drip: chronic sinusitis or allergic rhinitis sending protein-rich secretions into the oropharynx
- Lower GI: gastroesophageal reflux (GERD) sending acidic stomach contents and undigested protein back up into the esophagus and oropharynx
Differences from body odor:
- Can occur at any age (children through the elderly)
- Closely tied to diet, sleep, stress, medications, and chronic disease
- Physical interventions (such as squeezing out tonsil stones) only address the immediate symptom, not the underlying supply
- No single surgery can "cure" all sources — the dominant cause must be identified before triage
3. Why does this distinction matter so much?
Because different mechanisms mean fundamentally different treatment paths. If you treat breath odor as "just needing another cleaning and another bottle of mouthwash," you will likely:
- Keep cycling through dentistry when the real driver is in ENT (post-nasal drip) or GI (GERD)
- Expect a "one-time fix that never comes back" — but the oral microbiome is dynamically regulated, and the realistic goal is to reduce odor to a level that no longer bothers you, and maintain it
- Overlook diet, salivary flow, and medications, which are the genuinely modifiable amplifying factors
The first step at the Integrated Odor Clinic is to clarify which dominant source is driving your breath odor — not picking a tool first, but understanding the question first.
What are the 5 main sources of breath odor, and how do you tell them apart?
Five main sources: tongue coating, periodontal disease, tonsil stones, post-nasal drip, and GERD — each has a different odor signature and typical setting, and most people have a "primary source plus 1–2 secondary," so a recognition framework is needed to identify the main one first.Below is the framework most commonly used during initial consultations to identify the 5 main sources. Most people present with a "primary source + 1-2 secondary sources" pattern.
Source 1: Tongue coating (VSC-dominant)
Mechanism: anaerobic bacteria (Solobacterium moorei, Fusobacterium spp., etc.) on the posterior third of the tongue dorsum break down food debris and shed epithelium, producing hydrogen sulfide (H₂S), methyl mercaptan (CH₃SH), dimethyl sulfide ((CH₃)₂S), and other volatile sulfur compounds — a classic "rotten" smell. Characteristics:- Visible white or yellow coating on the tongue when looking in a mirror, especially toward the back
- Most noticeable upon waking (reduced salivary flow overnight plus a closed mouth)
- Temporarily improves after drinking water or eating
- Tongue brushing produces an immediate drop in odor intensity
Source 2: Periodontal disease / caries
Mechanism: anaerobic bacteria within periodontal pockets (Porphyromonas gingivalis, Tannerella forsythia, Treponema denticola — the "red complex") form biofilms; deep caries and faulty restorations provide protein sources — chronic inflammation plus protein breakdown produces odor. Characteristics:- Gums bleed easily, blood seen on the brush
- Loose or sensitive teeth
- Persistent odor, with limited improvement after brushing
- Deep plaque accumulation, presence of tartar
Source 3: Tonsil stones (tonsilloliths)
Mechanism: calcified food debris, shed epithelial cells, and bacteria accumulating within the tonsillar crypts (cryptae tonsillares) — containing a high concentration of sulfur compounds. Characteristics:- Occasional coughing up of small white or yellow lumps, with an intense odor
- Sensation of a foreign body deep in the throat
- Odor comes in waves, synchronized with the dislodging of tonsil stones
- Regular brushing and rinsing cannot reach the affected area
Source 4: Post-nasal drip
Mechanism: chronic sinusitis or allergic rhinitis produces postnasal mucus; protein-rich secretions enter the oropharynx and are metabolized by oropharyngeal bacteria, producing odor. Characteristics:- Thick secretions in the throat in the morning, frequent throat-clearing
- Nasal congestion, runny nose, history of allergic rhinitis
- Symptoms worsen when lying flat (nocturnal drip)
- Chronic cough (especially at night or in the morning)
Source 5: Gastroesophageal reflux disease (GERD)
Mechanism: acidic stomach contents (including partially undigested protein) reflux into the esophagus and oropharynx — accompanied by heartburn and belching, producing a sour-acidic odor (distinct from the "rotten" smell of the tongue-coating subtype). Characteristics:- Most noticeable 1-2 hours after meals or when lying down
- Heartburn, belching, regurgitation of sour fluid
- Odor leans more "sour" and "metallic"
- Often associated with esophagitis or pharyngitis
What multi-source coexistence actually looks like
| Comorbid pattern | Typical presentation |
|---|---|
| Tongue coating + periodontal (most common) | Worse in the morning, improves after brushing but returns within 2-3 hours, gums bleed |
| Tongue coating + post-nasal drip | Chronic nasal congestion + morning throat secretions + thick tongue coating |
| Tonsil stones + periodontal | Occasional coughing up of white specks + deep plaque accumulation |
| GERD + tongue coating | Sour smell after meals + rotten smell in the morning |
| All 5 sources (rare) | Usually combined with chronic disease, medication history, or low salivary flow |
What are the 5 common clinical archetypes of breath odor?
Five common archetypes: tongue-coating dominant, periodontal dominant, sinus/post-nasal-drip dominant, GERD-related, and a gray zone where you smell it but no objective source is found — matching yourself helps find which source and direction to start with.Twenty years of clinic work has surfaced 5 recurring archetypes of breath odor. Matching yourself to one can help identify where to start.
| Archetype | Typical presentation | Main source | Starting point |
|---|---|---|---|
| A. Morning-type | Worst on waking, improves after eating | Tongue coating (reduced overnight saliva) | Tongue brush + reinforced bedtime cleaning |
| B. Chronic-persistent | All-day odor, limited improvement from brushing | Periodontal / tonsil stones | Refer to periodontics or ENT for evaluation |
| C. Episodic-burst | Odor flares after coughing up white specks | Tonsil stones | ENT cryptolysis evaluation |
| D. Postprandial-sour | Worsens 1-2 hours after meals, with heartburn | GERD | GI evaluation + dietary adjustment |
| E. Strongly perceived by self but not others | Strong subjective sense, normal objective findings | OlRS grey zone | See Section 7 for details |
In real life, multiple archetypes often overlap — for instance, an A-type morning pattern coexisting with a B-type chronic pattern. The Integrated Triage first identifies the dominant source, then addresses the secondary contributors in sequence.
How do you run the 4-week home tongue-coating SOP for breath?
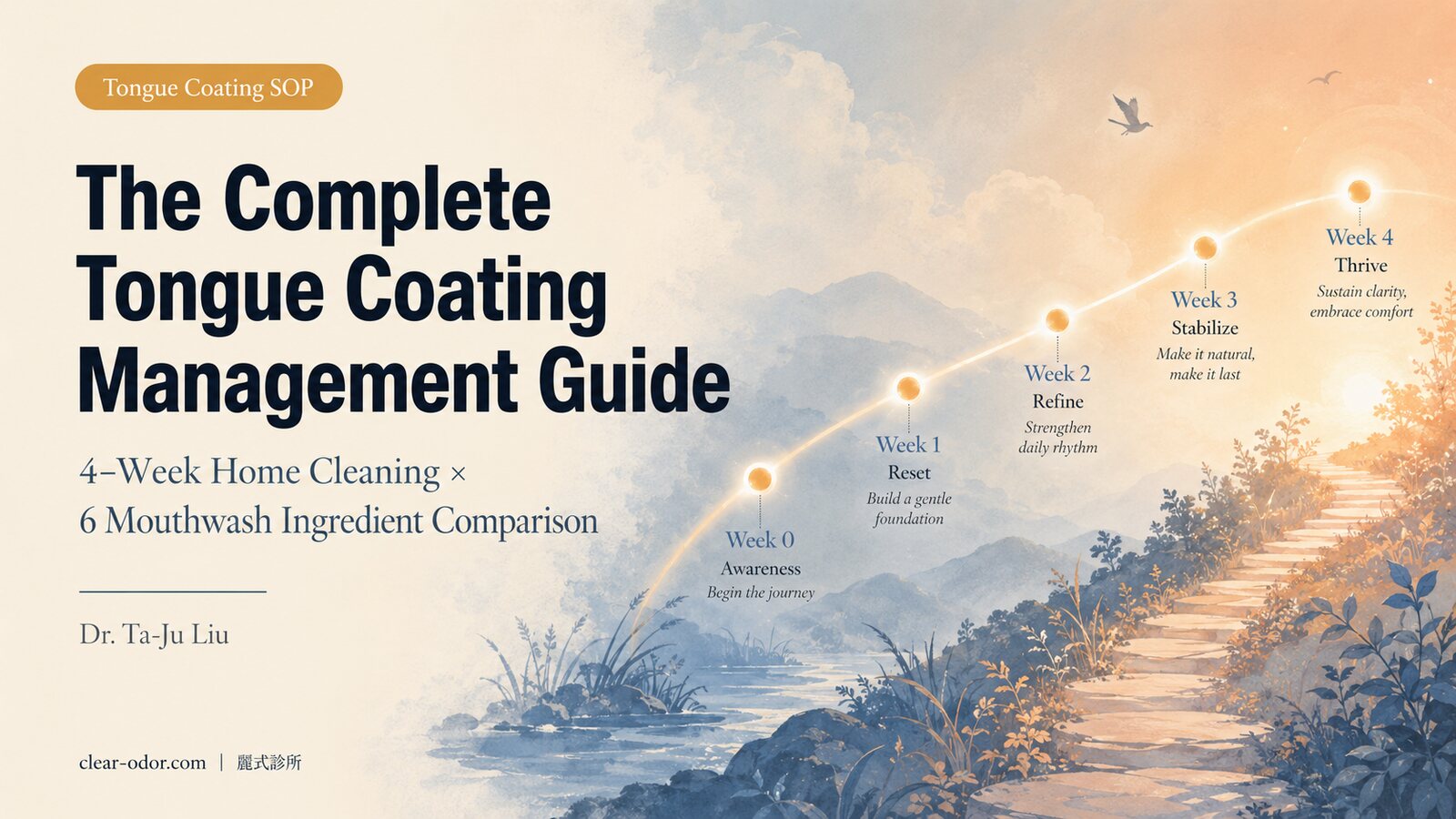
Tongue coating accounts for 60–70% of breath odor and is the easiest to track at home: use a 4-week systematic SOP — correct scraping, the right mouthwash ingredients, and logging odor at weeks 0/2/4 — and most people can gauge improvement first, then decide on medical intervention or referral.The tongue-coating subtype accounts for 60-70% of breath odor cases — making it the most common, and also the easiest source to observe improvement on through home management. Before any medical intervention, most people can start with a 4-week systematic plan.
Please record at Weeks 0 / 2 / 4:
- Self-rated odor intensity (0-10 scale)
- Tongue coating surface area (take a photo with the tongue extended, fixed lighting and angle)
- Associated symptoms (dry mouth, saliva thickness, sticky throat in the morning)
- Triggers (stress / medications / diet / lack of sleep)
Week 0: baseline recording + product inventory
- List all toothpastes, mouthwashes, and rinses you currently use, with ingredients
- Take a tongue-coating photo (suggested: before brushing in the morning, natural light, tongue extended as far as possible)
- Record current brushing frequency, whether you floss, whether you clean your tongue
- Self-rate odor intensity + note which times of day are worst
Weeks 1-2: building tongue cleaning technique
Key points for tongue scraping (the part most people get wrong):| Step | Detail | Common mistake |
|---|---|---|
| 1. Choose the tool | Silicone tongue scraper or stainless-steel scraper (avoid scraping with a stiff-bristle toothbrush) | Using a regular toothbrush to scrape — triggers the gag reflex |
| 2. Cleaning range | Scrape from the back of the tongue dorsum forward, especially the posterior third | Only scraping the tip — but the main anaerobic bacteria are at the back |
| 3. Pressure and frequency | Light to moderate pressure, 5-8 strokes per session, 1-2 times daily | Scraping until it bleeds — damages the papillae and worsens inflammation |
| 4. Timing | When brushing in the morning + before bed | Only doing it in the morning — but odor peaks overnight |
| 5. Combined rinse | Short course (1 week) of chlorhexidine 0.12% or essential-oil mouthwash | Daily long-term use — alters the oral microbiome |
- Morning: floss → brush → tongue scrape → therapeutic mouthwash (30 seconds)
- Evening: brush → tongue scrape → mouthwash
Week 3: salivary flow and lifestyle factor adjustment
Saliva is the body's natural antibacterial fluid and key to clearing food debris — insufficient saliva amplifies the tongue-coating subtype.
Reduce:- Excessive caffeinated drinks (dehydration, salivary suppression)
- Alcohol
- Sugary drinks (feeds bacteria)
- Smoking (directly reduces saliva and alters the microbiome)
- Fluids: 1.5-2 L per day (don't wait until thirsty)
- Sugar-free gum (10-15 minutes of chewing stimulates saliva)
- Zinc supplementation (linked to suppression of VSC production; use only under physician guidance)
Week 4: evaluation + next-step decision
| Improvement | Next step |
|---|---|
| ≥ 70% improvement | Maintain the current plan, transition to a stable maintenance rhythm (see Section 9) |
| 30-70% improvement | Fine-tune mouthwash ingredients and scraping technique, observe for another 2 weeks |
| < 30% improvement | Book an Integrated Triage evaluation, consider other coexisting sources |
| No improvement + obvious bleeding / loose teeth / swelling | See a dentist immediately — possible periodontal disease or other condition |
After home care doesn't work, what are the medical intervention tiers?
Medical intervention starts only after 4 weeks of home care show no change, on a "minimum strength, right specialty, regular re-evaluation" principle: Tier 1 prescription mouthwash or local measures, Tier 2 source-directed treatment in periodontics/ENT/GI, Tier 3 stubborn or multi-source integration — one tier at a time.If the 4-week home plan produces no improvement, you move into medical intervention. The principle is "minimum effective intensity, the right specialty, regular re-evaluation."
Tier 1: in-clinic management + basic dental care
| Intervention | Suitable for | Expected timeline |
|---|---|---|
| VSC volatile sulfur compound breath test | Objectifying odor intensity | Immediate reading |
| Tongue coating index assessment + education refresh | Home technique not yet dialed in | 2-4 week re-evaluation |
| Professional dental cleaning | Visible plaque / tartar | 1-2 sessions |
| Short course of chlorhexidine 0.12% | Acute periodontal inflammation | 1-2 weeks |
Tier 2: cross-specialty referral
Periodontics (if Tier 1 dental findings reveal deeper issues):- Pocket depth ≥ 4 mm → non-surgical periodontal therapy (deep cleaning, root planing)
- Pocket depth ≥ 6 mm + bone loss → periodontal surgery evaluation
- Faulty restorations / deep caries → re-fabrication / root canal therapy
- Recurrent tonsil stones → laser cryptolysis or tonsillectomy evaluation
- Chronic sinusitis → sinus CT + endoscopy, FESS if indicated
- Allergic rhinitis → nasal sprays (intranasal steroids) + antihistamines
- Endoscopic evaluation of esophagitis severity
- 24-hour pH monitoring (for atypical presentations)
- Medications: PPIs, H2 blockers, prokinetics
- Lifestyle adjustments: dinner-to-bedtime interval, elevating the head of the bed, weight management
Tier 3: advanced evaluation and multi-source integration
When Tier 1 + 2 treatment for 8-12 weeks still produces no improvement or relapses repeatedly:
- Microbiome testing (oral microbiome analysis): quantifying anaerobic bacterial composition
- Salivary function assessment: flow rate, buffering capacity, pH
- Rare differential diagnoses: characteristic breath odors of diabetic ketoacidosis, liver failure, kidney failure, trimethylaminuria (fish-odor syndrome) and other metabolic diseases
- Multi-source integration meeting: joint planning of treatment sequence with periodontics, ENT, and GI (a very small number of complex cases)
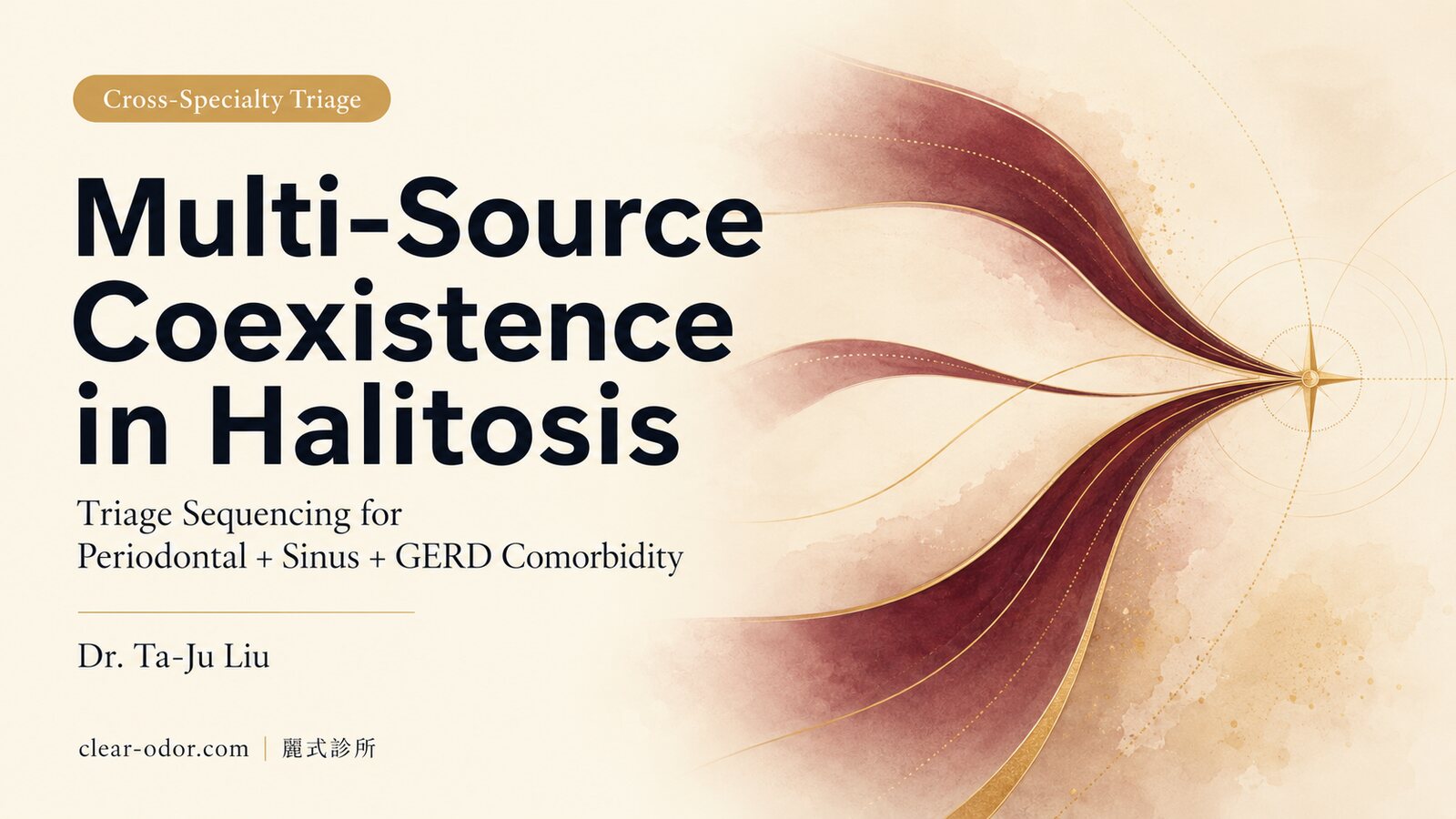
Why does starting with Integrated Triage save time vs a single specialty?
Because with multiple sources at once, a single specialty tends to look for the answer in its own field and miss the real primary cause — Integrated Triage sorts the primary source and comorbidities first, then refers in order to periodontics/ENT/GI, compressing months of guesswork into a sequenced plan.This is one of the most-asked questions in clinic. The short answer: when multiple sources coexist, a single specialty tends to look for the answer within its own field and miss the dominant cause.
Three core reasons
1. Multi-source coexistence is not rareRoughly 30-40% of patients with chronic bad breath have a "primary source + 1-2 secondary sources" pattern (e.g., periodontal + post-nasal drip, or tongue coating + GERD). If you book a purely dental visit first, get a cleaning, treat the periodontal issues, and see a 50% improvement but the odor persists — you may need another 1-2 months before suspecting "could it be something else?"
2. The cost of cross-specialty referrals is underestimatedGoing from dentistry → ENT → GI takes 4-8 weeks for one full loop (each specialty requires its own evaluation, exams, and treatment observation period). An Integrated Triage uses objective indicators at the initial visit (VSC test, tongue coating index, gingival bleeding index, history of nasal congestion, postprandial symptoms) to read out multi-source priority in one go, and issues referral letters directly to the appropriate specialties — typically saving 2-3 months of trial-and-error.
3. The "you're fine, off you go" negative loopMany patients describe being told "dentistry says you're fine, ENT says you're fine — but my breath still bothers me." This usually means an OlRS grey zone, or that the dominant source is in a specialty that hasn't been evaluated. The value of an Integrated Triage is striking the balance between "not missing anything" and "not overtreating."
Exceptions: when going straight to a single specialty makes sense
- Obvious periodontal symptoms (bleeding, loose teeth, pus) → straight to dentistry
- Obvious tonsil stone history (repeatedly coughing up white specks) → straight to ENT
- Obvious GERD symptoms (heartburn, acid regurgitation, nocturnal cough) → straight to GI
- Pure morning-type + clearly visible tongue coating (everything else normal) → try the 4-week home plan first, evaluate if it doesn't work
Integrated Triage isn't "something everyone needs to do." It's the right choice when you're not sure which specialty to book, or when you've already been cycling for 3+ months with no improvement.
"I think my breath is really bad, but everyone says it isn't" — what's going on?
This may be Olfactory Reference Syndrome (OlRS): a small group strongly feel they have bad breath, yet objectively family and friends notice nothing and exams find no source — here hunting for an "even stronger mouthwash or treatment" won't help; what's needed is a different kind of evaluation and support.A small number of patients describe "I feel my breath is really bad, but my family and friends say they don't smell anything" — this falls within the grey zone of Olfactory Reference Syndrome (ORS / OlRS).
Why this needs special handling
Jumping directly to "it's psychological, it's all in your head" causes two kinds of harm:
- A real physiological microbiome imbalance may be missed (subjectively strong + objectively mild is possible — e.g., tongue coating at the very back is hard to see yourself, but the odor genuinely exists)
- Patients who feel labeled find it even harder to seek help
The Integrated Odor Clinic approach:
Step 1 — Objective assessment to rule out physiological causes- VSC volatile sulfur compound breath test (quantified reading)
- Tongue coating index (standardized grading)
- Periodontal assessment (bleeding index, pocket depth)
- Third-party odor evaluation (medical staff + family member double-blind confirmation if needed)
- We do not conclude "it's psychological" — instead we explain that "objectively, the physiological assessment is normal; the subjective concern may have other contributing factors"
- Suggest pairing with a psychosomatic medicine or psychiatry evaluation (especially when accompanied by social avoidance or compulsive checking behaviors)
- ORS is classified within the OCD spectrum in DSM-5 and has dedicated treatments (CBT, SSRIs)
Even when objective findings are normal, the 4-week home tongue-coating plan has virtually no side effects and may improve subjective experience — this is far more helpful to patients than "we can't treat you."
Once the Phase 4 Integrated Evaluation flow goes live, OlRS screening will be built into the initial consultation process.
When should you book the integrated clinic instead of trying another mouthwash?
When 4 weeks of home care show no improvement, when you've seen a single specialty but odor remains, when it affects your social life, or when you're unsure which primary source you have — it's time to book Integrated Triage rather than trying one mouthwash after another.If any of the following is true → book an Integrated Triage rather than trying yet another mouthwash:
- You've already seen a dentist + had cleanings + tried multiple mouthwashes, but your breath is still bothering you
- You have nasal congestion / post-nasal drip / acid reflux at the same time, and you're not sure which specialty to book
- Family or coworkers have pointed out an odor, but you don't notice anything after brushing
- You subjectively feel a strong odor that others don't notice (OlRS grey zone evaluation)
- You also have odor in other areas (underarms, scalp, feet) that needs integrated handling
- Less than 30% improvement after the 4-week home tongue-coating plan
Integrated Odor Clinic initial consultation flow:
- History-taking (10-15 min): odor history, family history, lifestyle, medications, diet, salivary flow concerns
- Objective examination (10 min): VSC breath test, tongue coating index, gingival bleeding index, visual inspection of tonsillar crypts
- Odor assessment (5 min): clinician-side smell evaluation, with a third-party companion if needed
- Integrated plan (5-10 min): list a personalized Tier 0-3 path based on the assessment + issue referral letters to the appropriate specialties
After it improves, how do you maintain across 3/6/12 months without relapse?
Breath odor is about "stable maintenance," not "one-time cure": after improvement, keep the most effective cleaning and ingredients as routine, re-evaluate at 3 months, fine-tune at 6, and confirm stability at 12 — a maintenance rhythm prevents relapse better than a one-off sprint.Integrated odor care is about "stable maintenance," not "a one-time cure." Suggested long-term cadence:
3-month checkpoint
- Self-rated odor intensity: compared to baseline
- Progress on referred specialty treatments (periodontal maintenance, ENT follow-up, GI medications)
- Lifestyle factor review: have diet, sleep, stress, and hydration drifted back to old habits?
- Is the daily tongue-cleaning routine still being maintained?
6-month checkpoint
- Repeat objective assessment (VSC test, tongue coating index)
- Seasonal adjustment: dry winter air requires salivary attention; summer cold drinks require dietary attention
- Re-evaluate whether odor has appeared in other body areas (integrated perspective)
12-month checkpoint
- Full-year review: which months worsened, and the link with life events
- Long-term maintenance fine-tuning: whether you can move into a "minimum maintenance" mode (e.g., mouthwash dropping from daily to 2-3x per week)
- Overall health re-assessment: hormones, metabolism, and chronic disease medications — any changes?
FAQ — 12 of the most-asked decision criteria in clinic
Q1. Will Lis Clinic treat my breath odor directly?
Partly directly, partly via referral. Tongue-coating management + education + multi-source integration (the 4-week home plan) we handle directly; periodontal disease, tonsil stones, post-nasal drip, and GERD we evaluate first and then refer to trusted periodontists, ENT, and GI specialists. The point is to find the right source first, so you don't keep cycling within the wrong specialty.
Q2. Why not just book dentistry or ENT directly?
You can — but if you fall into the "multi-source coexistence" or "not sure which specialty to book" category, starting with an Integrated Triage can save trial-and-error time. About 30-40% of people with breath odor concerns have multiple sources (e.g., periodontal + post-nasal drip), and a single specialty tends to look for answers within its own field and miss the dominant cause.
Q3. Can breath odor actually be "cured"?
It depends on the source. The tongue-coating subtype can usually see substantial improvement through the 4-week home plan; the periodontal subtype can also improve significantly with professional treatment plus maintenance; tonsil stones and GERD require structured treatment plus lifestyle adjustments; the OlRS grey zone needs a different approach altogether. We don't use absolutist language — the goal is to reduce odor to a level that neither you nor the people around you find bothersome.
Q4. I've had tonsil stones squeezed out before, but they keep coming back — what now?
Common reasons for recurrent tonsil stones: (1) deep crypts that easily accumulate debris; (2) chronic tonsillitis; (3) insufficient saliva; (4) ongoing protein supply from post-nasal drip. After evaluation at our clinic, we discuss with ENT whether to consider cryptolysis or tonsillectomy — this is not a one-size-fits-all decision and needs to be led by ENT.
Q5. Is the clinic suitable for children / teenagers with breath odor?
Suitable for teenagers (junior-high and above). Breath odor in elementary-school-age children is mostly about personal hygiene (incomplete brushing, no tongue cleaning), and we suggest education and observation first. In teenagers, if there's increased sebum production from puberty, there may simultaneously be scalp- or face-related microbiome issues — these can be handled together in an odor-map framework.
Q6. I feel a strong odor but others don't — what should I do?
This may fall into the "Olfactory Reference Syndrome (OlRS)" grey zone. We start with objective testing (VSC volatile sulfur compound test + tongue coating index + periodontal assessment) to rule out physiological causes. If the full objective workup is normal but subjective concern persists, we suggest pairing with a psychosomatic medicine evaluation. Please mention this when booking via LINE so we can allocate adequate consultation time.
Q7. Can mouthwash "cure" bad breath?
No. Mouthwash (especially prescription-grade chlorhexidine formulations) can short-term suppress bacteria and reduce VSC production, but it cannot address structural issues (periodontal pockets, tonsillar crypts, post-nasal drip, GERD). Long-term daily chlorhexidine use also changes the oral microbiome, yellows the tongue coating, and alters taste — most clinical guidance recommends a 1-2 week short course followed by switching back to a regular fluoride or alcohol-free formula.
Q8. I've been using expensive toothpaste and active-ingredient mouthwash — why no improvement?
Toothpaste and mouthwash primarily address "surface-level" odor sources. If your dominant source is: (1) deep within periodontal pockets → needs professional cleaning and root planing; (2) tonsillar crypts → needs ENT; (3) post-nasal drip → needs ENT treatment of sinusitis; (4) GERD → needs GI intervention — no toothpaste, however expensive, can reach those places. Do the Triage first to find the dominant cause, then you'll know whether your tools are aimed in the right direction.
Q9. Do chlorophyll-based oral deodorant tablets actually work?
Limited. Oral deodorant tablets containing chlorophyll, mint, or parsley primarily act as "odor masks," with effects typically lasting 30-60 minutes. They're fine for occasional situations (an important meeting, before a date), but long-term reliance masks the underlying issue and delays root-cause treatment. Use them as an adjunct, not as the primary treatment.
Q10. Does smoking directly cause breath odor?
Yes — through multiple mechanisms: (1) tobacco residue retained in the oral mucosa; (2) reduced saliva, amplifying the tongue-coating subtype; (3) altered oral microbiome, increased periodontal disease risk; (4) chronic mucosal irritation. Most people see noticeable improvement 4-8 weeks after stopping (assuming other sources are also addressed).
Q11. Could my breath odor be related to my stomach?
Possibly. GERD (gastroesophageal reflux) is one of the 5 main sources, characterized by worsening 1-2 hours after meals along with heartburn and a sour taste. But not every "the stomach feels off" presentation is GERD — postprandial bloating is not necessarily acid reflux and needs GI evaluation. Rarer sources (such as H. pylori infection, liver failure, diabetic ketoacidosis) have their own characteristic odors and are considered during Tier 3 differential diagnosis.
Q12. What does the Integrated Triage evaluation flow look like?
You book an "Odor Map initial consultation" via LINE; the face-to-face visit covers: (1) detailed history of breath-odor-related issues and lifestyle; (2) objective testing (VSC, tongue coating, periodontal, tonsillar inspection); (3) listing the dominant and secondary sources in priority order; (4) drafting a personalized Tier 0-3 plan and issuing referral letters to the appropriate specialties as needed; (5) 4-8 week re-evaluation. Fee and duration are individualized in consultation based on your described situation.
Related Reading
- Tongue Coating & Bad Breath: A 4-Week Cleaning Guide
- When Bad Breath Has Many Sources: Gums, Sinus & GERD
- Bad Breath Despite Brushing? It's Usually Not Your Stomach
- Others Say You Smell but You Can't? Real vs Pseudo Odor
- Scalp Odor After Washing? The Microbiome & How to Manage
- Oral / Halitosis Integrated Triage
- Midlife Body Odor & Aging Odor Guide
A Closing Note
Breath odor is something many people quietly carry on their own, yet it is rarely discussed systematically. The root of it is not "finding the right toothpaste" as a single-point fix — it lies in understanding that multiple sources can coexist, and building a framework that starts with a Triage, then routes to the right specialty, then re-evaluates on a regular cadence.
The core stance of the Integrated Odor Clinic is this: odor is a signal, not a defect. It tells you that something somewhere in the body is out of balance — perhaps the oral microbiome, perhaps the nasopharynx, perhaps the GI tract, perhaps a layering of several sources. Clarifying that signal matters more than covering it up.