
When it comes to body odor and bad breath, there are two opposite — yet equally distressing — situations:
- One is: "My family or coworkers say I have an odor, but I can't smell anything at all — is it really true?"
- The other is: "I keep feeling I have bad breath or body odor, but everyone around me says, 'No, I don't notice anything' — am I overthinking it?"
These two seem contradictory, but each has a clear reason behind it. The first is usually olfactory adaptation — we go "nose-blind" to a smell that's always there around us; the second may be pseudo-halitosis, and in a few cases even a life-disrupting anxiety about "sensing an odor." This article aims to explain this hard-to-talk-about topic with empathy and without shame.
Not sure whether the odor is real or where it's coming from? You can first use the Midlife Body Odor & Aging Smell Integrated Guide to identify the source, then come back to this article for the question of "can I smell it myself or not."
Why can't you smell your own odor?
Because of olfactory adaptation — when a smell is constantly present, the smell receptors gradually turn down their response, so "you can't smell it" does not mean "there's no odor.""I'm with myself all day — how could I not smell my own odor?" — That's exactly the point.
Smell Receptors Turn Down Their Response to a Constant Odor
The human sense of smell has a feature called olfactory adaptation: when a smell is constantly present, the smell receptors gradually "turn down their response," so you smell it less and less. This is why:
- When you walk into someone else's home, you notice "their home's smell," but you can't smell "your own home's smell";
- After you put on perfume, you stop noticing it yourself after a while, but others smell it the moment they get close;
- Your own body odor and breath, because they're there all day, are precisely the ones you're least likely to notice yourself.
"Can't Smell It" Doesn't Mean "There's No Odor"
So — "I can't smell it" does not mean "there's no odor." This isn't because you're insensitive or don't care; it's the normal physiology of smell. That's also why a family member's heads-up is often more accurate than your own perception — and why so many cases of midlife body odor are "first noticed by a partner."
"Others can smell it" vs. "I feel I smell bad" — are these the same thing?
No. One is where others smell it but you can't (usually olfactory adaptation); the other is where you feel you smell bad but others can't (possibly pseudo-halitosis or anxiety about sensing an odor) — and the two call for completely different approaches.| Situation | What you feel | What others feel | More likely cause |
|---|---|---|---|
| A | I can't smell it | Others say there's an odor | Olfactory adaptation (the odor is real, you've just grown used to it) |
| B | I feel I smell bad | Others say they don't notice | Pseudo-halitosis, or anxiety about sensing an odor |
The Two Situations Call for Completely Different Approaches
- Situation A: The odor is usually real, and the focus is on finding the source and treating it accordingly (mouth? aging skin odor? scalp? residue on clothing?).
- Situation B: Objectively, others can't smell it, and the focus is on first confirming with objective methods, then deciding whether to keep seeing a dentist, or whether psychological support is actually what's needed more.
Figuring out which one you fall into is the most important first step in this article.
How do you tell real bad breath from pseudo-halitosis?
Medically there are three: genuine halitosis (others can smell it too), pseudo-halitosis (you strongly feel it but objective checks and others can't), and halitophobia (exams are normal yet you can't believe it) — and the latter two are real conditions, not "overthinking."Medically, bad breath (halitosis) is actually divided into a few situations:
The Three Medical Categories
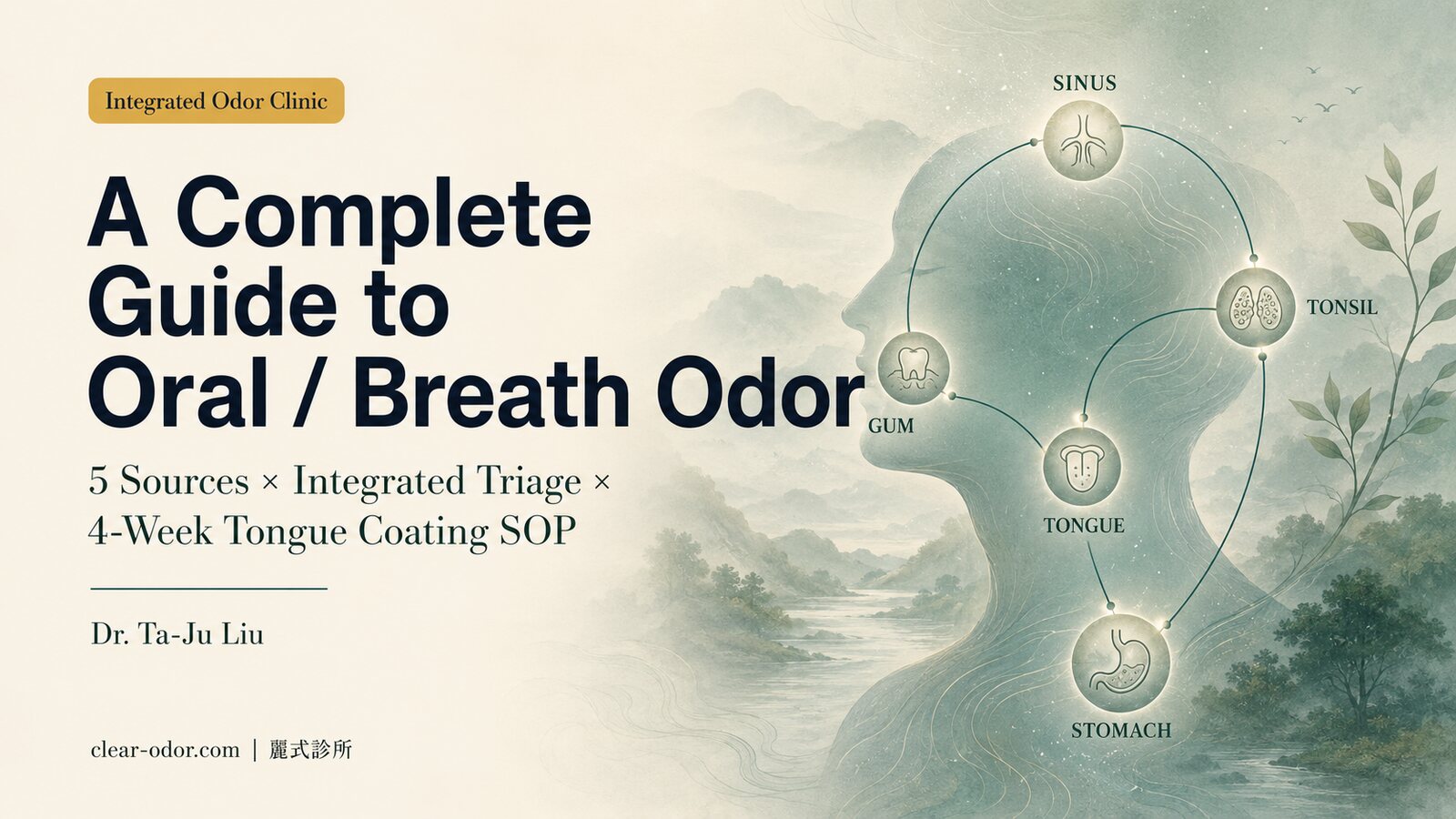
- Genuine halitosis: Bad breath that objectively exists and that others can also smell. Most of it comes from the mouth (tongue coating, gum disease, tonsil stones, etc.), and a smaller portion from outside the mouth or from the body as a whole. For the sources and management of this part, see Bad Breath That Won't Go Away Even With Brushing.
- Pseudo-halitosis: The person strongly feels they have bad breath, but objective examination and the people around them can't smell anything.
- Halitophobia: Even when both examination and the people around them confirm there is no bad breath, the person still can't believe it and keeps worrying.
These Are Real Conditions, Not "Overthinking"
Pseudo-halitosis and halitophobia are real conditions, not "overthinking" or "being dramatic." They can make people afraid to talk close to others, repeatedly check their breath, and over-brush and over-rinse — and in severe cases, they affect social life, work, and emotional well-being. Understanding that this is real is the first step toward letting go of self-blame.
What if you keep feeling you smell bad but others say you don't?
When that feeling grows intense enough to bring repeated checking, social avoidance, and real suffering while others objectively can't smell anything, medicine describes it as Olfactory Reference Syndrome (ORS) — and this suffering is real, something that can be understood and supported.There's a situation that deserves especially gentle handling: a person is deeply convinced they give off an unpleasant body odor or breath — to the point of repeated checking, avoiding social situations, and real suffering — but objectively, the people around them can't smell anything. In medicine this is described as Olfactory Reference Syndrome (ORS) — an excessive anxiety about self-perceived body odor or bad breath.
Common Features of the Anxiety of Sensing an Odor
Its features often include:
- An overpowering belief in one's own odor: A strong belief that one has an odor others can smell, with no relief even after being reassured again and again;
- Repeated checking behaviors: Constant "checking" — smelling one's hands, smelling one's clothes, watching others' facial expressions, repeatedly brushing and washing;
- Avoidance for fear of being smelled: Avoiding social events, dates, meetings, and public transport for fear of being smelled.
Please Remember Two Things
If you or a family member experiences this, please remember two things: First, this suffering is real — it is not weakness or being dramatic; and second, for this kind of distress, mental-health care (psychiatry/psychology) and psychological support are often more helpful than endlessly switching mouthwashes. Treat it as a situation that can be understood and supported, not a shameful secret.
How can you objectively judge whether you actually have an odor?
Rather than cycling through anxiety by feeling, use relatively objective methods: ask someone you trust to judge honestly, do the wrist-lick test, check the back of your tongue in the mirror, and note the timing and context.Rather than cycling endlessly through anxiety over "do I smell or not," it helps to use a few relatively objective methods:
Four Relatively Objective Self-Check Methods
- Find one or two people you trust who will tell you the truth and ask them directly and privately to honestly judge for you — this is far more accurate than smelling yourself.
- The wrist-lick test: Lick the inside of your wrist, wait a few seconds for it to dry, then smell it (you're smelling the odor of dried saliva, which is more accurate than breathing directly onto your hand).
- Look at your tongue and tongue coating: In the mirror, check whether there's a thick coating on the back of your tongue — this is the single most common source of bad breath.
- Note the timing and context: Is it there all day, or only at certain times (morning, on an empty stomach, when your mouth is dry)? Is it from one specific spot, or "everywhere"?
How to Decide Your Next Step After Checking
If objective checks and people you trust both point to "there really is an odor," move toward finding the source and treating it accordingly; if they all say there's nothing, yet you remain intensely anxious, then that anxiety itself is what most needs care.
When should you see a dentist/doctor, and when should you seek mental-health support?
If others confirm an odor and you want to find the source, see a dentist first; when objective checks are normal yet you keep worrying intensely and avoiding social situations, mental-health and psychological support is often more helpful; if you can't tell, an objective evaluation first can confirm nothing has been missed.A simple triage principle:
Triage for Three Situations
- Others confirm there's an odor, and you want to find the source → See a dentist first (the largest category of bad breath comes from oral sources), and if needed, follow the clues to a dermatologist or an integrated odor evaluation.
- Objective examination is normal and others can't smell anything, yet you keep worrying intensely, checking repeatedly, and avoiding social situations → Here, the help of mental-health care (psychiatry/psychology) and psychological support is often more practical than switching to yet another mouthwash.
- It's a borderline case and you can't tell which one → You can first do one objective oral and integrated evaluation to "confirm nothing has been missed," then decide on the next step — sometimes "confirming there's no problem" is itself the starting point of peace of mind.
Whichever It Is, You Don't Have to Struggle Alone
Whichever it is, please don't struggle alone just because it's "hard to bring up." It's a concern many people have, and one that can be handled well.
Frequently Asked Q&A
Q1. Why does everyone say I have an odor when I can't smell it myself?
Because of olfactory adaptation: for your own smell that's constantly present all day, the smell receptors turn down their response, so you smell it less and less. This doesn't mean there's no odor — in fact, a family member's heads-up is often more accurate.
Q2. I keep feeling I have bad breath, but everyone says I don't — is something wrong with me?
It's not a simple "sick or not sick" split. When others objectively can't smell it but you strongly feel it's there, medicine calls this pseudo-halitosis or halitophobia — a real form of distress, not being dramatic. Confirm with objective methods first, then decide on a direction.
Q3. What's a more accurate way to test whether I have bad breath?
Asking someone you trust to judge honestly is the most accurate; next best is the wrist-lick test — lick, let it dry, then smell — and checking the back of your tongue in the mirror. Breathing directly onto your palm is actually unreliable.
Q4. Which kind of doctor handles the anxiety of sensing an odor (ORS)?
When objective examination is normal yet you keep worrying intensely and it affects your life, mental-health care (psychiatry/psychology) and psychological support are usually more helpful than repeatedly seeing a dentist. This suffering is real and deserves to be cared for well.
Q5. How do I tell a family member "you have an odor" without hurting them?
Put the focus on "handling this together" rather than blame — for example, start with changing pillowcases and clothing, or going to see a doctor together. The article Managing Body Odor on Clothing and Bedding offers concrete wording for caregivers.
Q6. Once I've confirmed there really is an odor, what's the next step?
Find the source and treat it accordingly: for breath, see a dentist first; for aging skin odor, see a dermatologist; if you're unsure, use the Midlife Body Odor Integrated Guide to identify the source, then decide whether to do an integrated evaluation.
A Final Note
"People say I have an odor but I can't smell it" and "I feel I smell bad but others say I don't" — these two opposite situations are both very common, and both have clear explanations and ways forward. The former is usually olfactory adaptation, where the focus is on finding the source and treating it accordingly; the latter may be pseudo-halitosis or the anxiety of sensing an odor, where the focus is on confirming with objective methods and seeking mental-health support when needed.
Most important of all: this is nothing to be ashamed of, and you don't have to struggle through it alone. Whichever situation you're in, you can be understood and supported well. If you'd like to figure out which one applies to you and what to do next, you're welcome to contact us online, and Dr. Ta-Ju Liu will help you sort out a direction based on your individual situation.
This article is integrated educational information and cannot replace a formal in-person consultation or professional psychological evaluation. If emotional distress is significant, we recommend seeking help from mental-health care or a psychological professional.
Bad breath can, in most cases, be traced and dealt with
Bad breath and oral discomfort can, in most cases, "be traced and dealt with." Our integrated team means both the in-mouth and outside-the-mouth sources of bad breath can be assessed and handled in-house: family physician Dr. Yen-An Lin focuses on burning mouth syndrome, bad breath, and oral health (in-mouth and metabolic sources); ENT specialist Dr. Wan-Chun Tsai (with a focus on oral conditions and aesthetic medicine) can assess outside-the-mouth sources such as the sinuses, post-nasal drip, and tonsil stones. Only when the issue is confirmed to be a dental structural problem (decay, periodontal treatment needed) do we help arrange a referral to dentistry. Sort out the source first, rather than rushing to blame the stomach.
If you've been bothered by long-standing bad breath or oral discomfort, you're welcome to book an assessment.
Related Reading
- Bad Breath Despite Brushing? It's Usually Not Your Stomach
- Bad Breath Brushing Won't Fix? 5 Sources & Which Doctor
- Clothes & Pillows Still Smell After Washing? How to Fix It
- Do Chinese Herbs Help Body Odor & Bad Breath? The Evidence
- You Smell but Others Don't? Olfactory Reference Syndrome
- Oral / Halitosis Integrated Triage
- Midlife Body Odor & Aging Odor Guide