
Why Does Tongue Coating Deserve Its Own Dedicated Article?
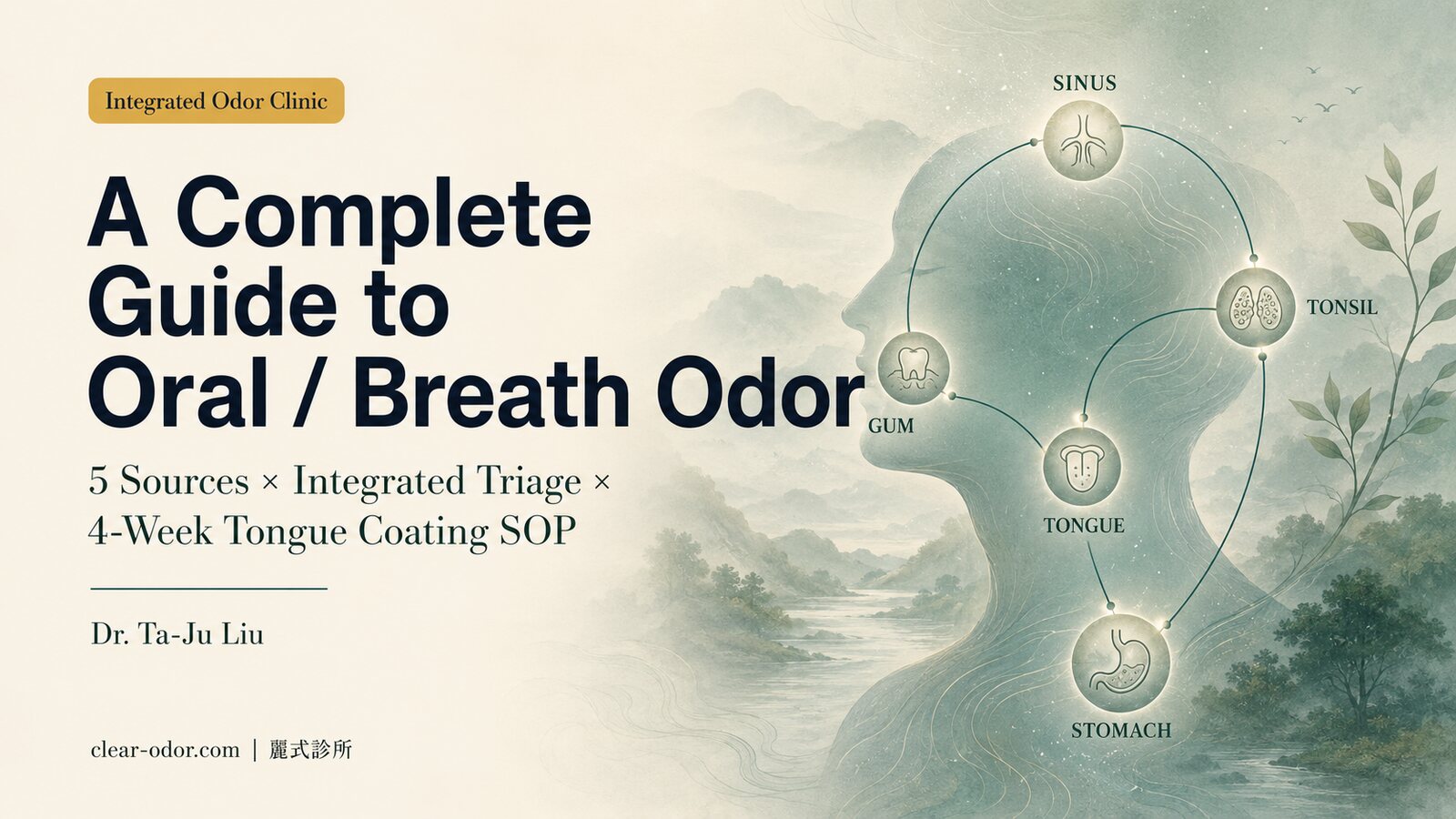
Oral malodor has at least five major source categories (tongue coating, periodontal, tonsil stones, post-nasal drip, GERD), but tongue-coating-driven cases account for 60-70% — making it the most common source, and also the one where home management most readily produces observable improvement.
The problem is that most people get three things wrong when "brushing the tongue":
- Wrong area: only brushing the visible tip, missing the core odor-producing zone (the posterior third of the dorsal tongue)
- Wrong tool: scraping with a regular toothbrush triggers the gag reflex, causing them to stop before reaching the back
- Wrong mouthwash: hearing that chlorhexidine is "strong" and using it daily, which over time alters the oral microbiome, yellows the tongue coating, and changes taste perception
This article distills the most frequently asked clinical judgments from the past 20 years in practice — the goal is to help you use the right method, identify your own type, and know when to step up to prescription care within 4 weeks.
Why does tongue coating smell? What are anaerobic bacteria and VSCs?
The papillae on your tongue form a ridged surface that traps food debris, shed cells, and saliva, giving anaerobic bacteria a low-oxygen place to thrive; those bacteria break down protein into volatile sulfur compounds (VSCs) — the main source of bad-breath odor.The tongue surface is covered with papillae, forming a microscopic "ridged structure" that naturally traps food debris, shed epithelial cells, and salivary components — providing a low-oxygen environment ideal for anaerobic bacteria to thrive.
Key Anaerobic Bacteria
- Solobacterium moorei: strongly associated with halitosis, regarded as an "indicator species" for bad breath
- Fusobacterium nucleatum: often co-exists with periodontal disease and cross-site infection
- Atopobium parvulum, Prevotella: strong VSC producers
- Tannerella forsythia: a red-complex member shared between tongue coating and periodontal disease
The Chemistry of VSCs (Volatile Sulfur Compounds)
Anaerobic bacteria break down sulfur-containing amino acids (cysteine, methionine) to produce:
| VSC compound | Formula | Odor character |
|---|---|---|
| Hydrogen sulfide | H₂S | "Rotten egg," most common |
| Methyl mercaptan | CH₃SH | "Rotting vegetables," most pungent |
| Dimethyl sulfide | (CH₃)₂S | "Rotting seaweed," also linked to GI sources |
VSCs can be detected by the human nose at the ppb (parts per billion) level — which is why you may perceive it as "faint" while others perceive it as "distinctly unpleasant".
Why the Posterior Third Is the Core Zone
The dorsal tongue can be divided into anterior, middle, and posterior thirds:
- Anterior third: frequently touched during tooth brushing, mechanically rubbed by food, and rinsed by saliva → anaerobes have a hard time accumulating
- Middle third: moderate exposure to cleaning
- Posterior third: the tongue retracts during brushing so this area is missed, papillae are deepest, and food residue and shed cells accumulate most → the zone producing the most VSCs
In other words: if your tongue scraper only reaches the tip, you have essentially not addressed the real odor-producing zone.
What are the 5 most common tongue-cleaning mistakes?
The five most common: using a toothbrush instead of a scraper, scraping too hard and injuring the papillae, only cleaning the tip and missing the back (where VSCs are highest), cleaning too infrequently, and cleaning without addressing dry mouth and saliva — wrong technique, and no amount of scraping controls the smell.Five common mistakes distilled from 20 years of clinical experience:
Mistake 1: Using a Regular Toothbrush to Scrape
Problem: Toothbrush bristles are designed for enamel hardness. Scraping the papillae causes inflammation, bleeding, and triggers the gag reflex — most people stop after one or two strokes. Fix: Use a silicone tongue scraper (soft, less likely to trigger gagging) or a stainless-steel tongue scraper (C-shaped, can reach the posterior region). Purpose-built tools (BreathRx, DenTek, etc.) are widely available and usually inexpensive.Mistake 2: Only Cleaning the Tip
Problem: The tip is what's visually obvious, but anaerobic bacteria concentrate in the posterior third. Fix: The cleaning range should start from the back and pull forward — extend the tongue as far as possible (use a mirror), place the scraper at the junction of the middle and posterior thirds, and pull forward. Rinse off the debris with water after each stroke. 5-8 strokes recommended.Mistake 3: Pressing Too Hard, Causing Bleeding
Problem: Heavy pressure damages the papillae and causes surface inflammation — and inflamed tissue actually accumulates more odor-causing material. Fix: Use light to moderate pressure, just enough to feel slight contact. If the tongue becomes red or bleeds after one session, halve the pressure next time.Mistake 4: Only Doing It in the Morning
Problem: Nighttime is when odor production peaks — the mouth is closed, saliva flow drops, and anaerobes are most active. Morning cleaning only removes what accumulated overnight; it doesn't slow daytime accumulation. Fix: Clean once when brushing in the morning, and once before bed. Bedtime cleaning lowers the overnight VSC baseline.Mistake 5: Not Rinsing at All, or Only Rinsing with Water
Problem: A complete protocol is physical cleaning (the scraper) + chemical suppression (mouthwash) — brushing alone allows the remaining anaerobes to return to baseline within 2-4 hours. Fix: After brushing and scraping, hold mouthwash in the mouth for 30 seconds. A short course (1-2 weeks) of chlorhexidine 0.12% or essential oils is fine; for long-term use, switch to a fluoride-based or alcohol-free, gentle formula. See the next section.Of the 6 mouthwash ingredients, which actually helps breath most?
Chlorhexidine, chlorine dioxide, zinc salts, CPC, essential oils, and alcohol each have a role: they differ in antibacterial power and ability to neutralize VSCs, with trade-offs like staining or irritation — for tongue-coating breath, ingredients that neutralize VSCs (zinc salts, chlorine dioxide) usually help more than ones that just feel "fresh."Mouthwash ingredients vary widely. The table below summarizes the characteristics and indications of the 6 most common active ingredients:
| Ingredient | Mechanism | Indications | Caveats |
|---|---|---|---|
| Chlorhexidine 0.12% | Broad-spectrum antibacterial, strong VSC reduction | Acute periodontal inflammation, short-term 1-2 weeks | Long-term use causes staining, alters microbiome, changes taste |
| Essential oils (Listerine, etc.) | Antibacterial, anti-inflammatory | Moderate strength, usable for 4-6 weeks | Alcohol-based formulas irritate mucosa; alcohol-free versions are gentler |
| CPC (Cetylpyridinium Chloride 0.07%) | Antibacterial, reduces biofilm | General daily use | Limited efficacy against certain bacteria; not sufficient alone |
| Zinc (Zn) compounds | Directly binds sulfur, reduces VSCs | Tongue-coating-type halitosis, suitable for long-term use | Mostly in combination products; fewer options available |
| Chlorophyll | Primarily odor masking | Occasional short-term use | Doesn't address the source; long-term reliance delays proper care |
| Oxygenating (active oxygen) | Inhibits anaerobic growth | Anaerobe-dominant cases (e.g., tongue-coating type) | Newer category, limited long-term data |
How to Choose
Week 1: Baseline assessment. Use a standard fluoride mouthwash (without special antibacterial agents) after brushing and scraping, and observe baseline odor intensity. From Week 2 onward: Choose based on the dominant mechanism —- Heavy tongue coating, strong VSCs → CPC or zinc formula, continuous use
- Acute periodontal inflammation → chlorhexidine 0.12% short course 1-2 weeks, then switch back to CPC
- Chronic, multi-source → essential oils at moderate strength for long-term use
- Want to try a newer category → oxygenating formula
What do you do each week of the 4-week home SOP?
Week 0 records your baseline (odor, coating thickness), Weeks 1–2 build correct scraping and rinsing habits, and Weeks 3–4 fine-tune tools and ingredients while tracking improvement — a measurable 4-week flow replaces blindly trying products and shows which step actually works.Week 0: Baseline Recording
- Photograph the tongue coating (before brushing in the morning, natural light, tongue extended as far as possible, fixed angle)
- Self-rate odor intensity (0-10 scale), noting which times of day are worst over the course of a week
- List the ingredients of all current oral care products
- Record water intake, caffeine intake, and smoking status
Week 1: Building the Technique
Daily routine:- Morning:→ Floss (clean between teeth) → Brush (fluoride toothpaste, 2 minutes) → Tongue scraper (back to front, 5-8 strokes, light to moderate pressure) → Mouthwash held for 30 seconds
- Before bed:→ Brush → Tongue scraper → Mouthwash
Week 2: Ingredient Intervention
Based on the baseline observed in Week 1, choose the corresponding mouthwash (see the table in Section 3). After 1-2 weeks of use, observe:
- Morning odor intensity (compared to Week 0)
- Tongue coating coverage (compare photos)
- Any side effects (mucosal irritation, taste change, color change of coating)
Week 3: Adjusting Lifestyle Factors
Saliva volume is the natural antibacterial and food-clearing mechanism — without addressing it, tongue scraping alone has limited effect.
Reduce:- Excessive caffeinated beverages
- Alcohol
- Sugary drinks
- Smoking
- Water: 1.5-2 L daily
- Sugar-free chewing gum (10-15 minutes of chewing)
Week 4: Evaluation and Next Steps
| Improvement | Next step |
|---|---|
| ≥ 70% | Maintain current plan, transition to a stable rhythm (mouthwash can drop to 3-5 times per week) |
| 30-70% | Fine-tune mouthwash ingredient, check tongue-scraping technique, observe another 2 weeks |
| < 30% | Schedule an Integrated Triage evaluation — there may be coexisting sources (periodontal, tonsil stones, post-nasal drip, GERD) |
After 4 weeks at home with no improvement, when should you see a doctor?
If 4 weeks of home care brings no clear improvement, or it comes with bleeding gums, periodontal problems, tonsil stones, or odor that actually comes from a non-tongue source, it's time to step up to prescription care or refer to periodontics/ENT — tongue coating is only 60–70% of breath odor; the rest needs the right specialty.When the home protocol shows no improvement, common escalation paths:
Stepping Up to Prescription-Grade Chlorhexidine 0.12%
Indications:- Acute periodontal inflammation (visibly swollen, bleeding gums)
- No improvement after 4 weeks of home protocol; considering a short course to break through
- Adjunct after extraction, implant, or periodontal surgery
Referral to Periodontics
Indicated when any of the following applies:
- Recurrent bleeding or swelling of the gums
- Tooth mobility
- Deep plaque accumulation, presence of calculus
- Persistent oral malodor with limited improvement after a dental cleaning
- No meaningful improvement after the 4-week home protocol plus a mouthwash step-up
Periodontics will perform:
- Periodontal pocket depth measurement (probing)
- X-ray assessment of bone loss
- Non-surgical deep cleaning (scaling and root planing) when needed
- Periodontal surgery evaluation in severe cases
Referral to Integrated Triage
If odor persists after a 4-week home protocol plus periodontal treatment, an Integrated Triage is recommended — other sources (tonsil stones, post-nasal drip, GERD) may coexist, and a single-specialty approach won't reach the root cause.
FAQ — 8 Most Common Clinical Questions
Q1. Does thicker tongue coating mean stronger odor?
Related, but not strictly proportional. Thicker coating usually reflects more anaerobic bacteria and shed epithelial cell buildup, but odor intensity is also affected by species composition — for example, two tongues with the same coating thickness can smell very differently if one has more Solobacterium moorei. Objective measurement (VSC breath testing) is more accurate than visual assessment of coating thickness.Q2. Why does the odor come back 2 hours after I scrape my tongue?
That's normal. VSCs return to baseline after each cleaning — the goal of cleaning is to "lower the rate of accumulation and the peak level," not to "stop production forever." Two daily cleanings (morning and evening) keep the daytime average VSC low. If strong odor returns within 2 hours, possible causes are: (1) technique not in place (the posterior third was missed); (2) insufficient saliva; (3) coexisting other sources.
Q3. The tongue scraper makes me gag. What do I do?
5 techniques: (1) switch to a silicone scraper (softer than a rigid scraper); (2) start from the middle and gradually work back; (3) breathe steadily through the nose, don't hold your breath; (4) do it before eating in the morning (gag reflex is weaker on an empty stomach); (5) practice for 1-2 weeks — most people adapt. If you truly cannot overcome it, use a scraper and work over shorter ranges with multiple passes.Q4. Do chlorophyll or mint lozenges actually work?
Limited effect. They primarily mask odor, with effects typically lasting 30-60 minutes. For occasional needs (important meetings, before a date), short-term use is fine — but long-term reliance masks the real problem and delays addressing the source. Treat them as adjuncts, not primary treatment.Q5. Can I use chlorhexidine mouthwash daily?
Not recommended. A short course of 1-2 weeks is fine, but long-term use causes: (1) staining of teeth and tongue; (2) taste changes; (3) shifts in the normal oral microbiome — which can actually worsen tongue coating; (4) mucosal irritation. Most clinical guidelines recommend switching back to a fluoride or CPC formula after the short course.Q6. My tongue coating has turned yellow / black. What's going on?
Possible causes: (1) staining from long-term chlorhexidine use; (2) microbiome shift after antibiotic treatment; (3) smoking; (4) staining from caffeinated drinks; (5) rarely, black hairy tongue (associated with heavy smoking, long-term antibiotic use, or poor oral hygiene). If accompanied by worsening odor or taste changes, an in-person evaluation is recommended.Q7. Can tongue coating be fully removed?
It cannot, and shouldn't be. A healthy tongue coating is a very thin, pale-white layer — this represents normal papillae and microbiome and is not pathological. The goal is to "reduce abnormal thickness (such as a thick yellow-white film or full coverage)," not to "scrape it clean." Aggressive removal damages the papillae and disrupts the normal microbial balance.Q8. What does the Integrated Triage process look like?
Initial visits are booked through LINE for the "Odor Map initial consultation," with integrated handling during the in-person session: (1) detailed history-taking around breath-related concerns and lifestyle; (2) objective measurements (VSC, tongue coating index, periodontal, tonsil inspection); (3) prioritization of primary and secondary sources; (4) personalized Tier 0-3 plan, with referral letters to corresponding specialties when needed; (5) re-evaluation visit at 4-8 weeks. Fee and duration are individualized in consultation based on your situation.
Related Reading
- Bad Breath Brushing Won't Fix? 5 Sources & Which Doctor
- When Bad Breath Has Many Sources: Gums, Sinus & GERD
- Bad Breath Despite Brushing? It's Usually Not Your Stomach
- Wash Hair Daily or Every Other Day? Scalp Microbiome
- Oral / Halitosis Integrated Triage
A Closing Note
Tongue coating management is the "first stop" in handling oral malodor — 80% of people see significant improvement within 4-8 weeks once they use the right method, the right tools, and the right ingredient pairing. But doing it right isn't about watching more YouTube tutorials — it's about using the right tools, cleaning the right areas, pairing the right mouthwash, and adjusting saliva volume.
If improvement is less than 30% after the 4-week plan, please book an Integrated Triage rather than continuing to try new products — the possibility of multi-source coexistence requires objective evaluation to rule out.