
"Doctor, I brush my teeth diligently every day, I even floss, but my mouth still has a smell — is it because my stomach is bad? I've been taking stomach medication for half a year."
This is the sentence most often asked out loud about bad breath in my clinic. The person asking has usually already been around the block: they've switched between several toothpastes, bought mouthwash, seen a gastroenterologist and had an endoscopy, been told "nothing's really wrong" — and yet the smell is still there, so present they have to keep a deliberate distance when talking to people.
This article wants to make one thing clear that a lot of people have misunderstood for a long time: bad breath that brushing won't get rid of usually isn't a stomach problem. About 80–90% of bad breath comes from inside your mouth — just in places a toothbrush can't reach. We'll unpack the five major oral sources one at a time, explain why "I try so hard to brush and it does nothing," how much weight GERD really carries, when you should actually look to the whole body, and — which doctor to see for bad breath.
Does bad breath come from the stomach? About 80–90% comes from the mouth
Bad breath is rarely the stomach's smell drifting up — it's manufactured on the spot by oral anaerobic bacteria, with about 80–90% of the source in the mouth and only a small fraction from the stomach.The takeaway: the odor factory is in the mouth, not the stomach
Let's start with the conclusion: according to halitosis research and clinical consensus, about 80–90% of bad breath originates in the mouth itself, with only a small fraction coming from the nasopharynx, the airway, or whole-body metabolism — and "the stomach" actually accounts for a very small proportion.
The chemical essence of bad breath is a group of gases called VSCs (volatile sulfur compounds) — mainly hydrogen sulfide (a rotten-egg smell), methyl mercaptan (a rotting-cabbage smell), and dimethyl sulfide. These gases don't appear out of nowhere; they are the metabolic exhaust produced when anaerobic bacteria in the mouth break down protein residue (shed oral mucosal cells, food debris, blood cells, and proteins in saliva). Wherever it's low in oxygen, wherever protein residue gets trapped, wherever the brush can't reach — that's where odor-producing anaerobic bacteria thrive.
Once you understand this, the whole thing falls into place: bad breath isn't "the smell from the stomach drifting up" — it's an odor manufactured on the spot by bacteria in the mouth. That's why so many people take stomach medication for half a year with no result — the direction was wrong from the start; the drug acts on the stomach, but the odor factory is in the mouth.
Key takeaway: The essence of bad breath is the VSCs (volatile sulfur compounds) produced when oral anaerobic bacteria break down protein residue. About 80–90% of bad breath originates in the mouth, not the stomach. Checking the mouth thoroughly first is the most efficient first step in dealing with bad breath.
Why you often can't smell it yourself
There's also a commonly overlooked physiological phenomenon: people can't smell their own breath (olfactory fatigue). With long-term exposure to your own scent, the brain treats it as background and automatically filters it out. So "I don't smell anything" and "my family says it's strong" often hold true at the same time — nobody is exaggerating; this is just a feature of the sense of smell. It's also why bad breath is usually noticed by others first and by the person themselves last.
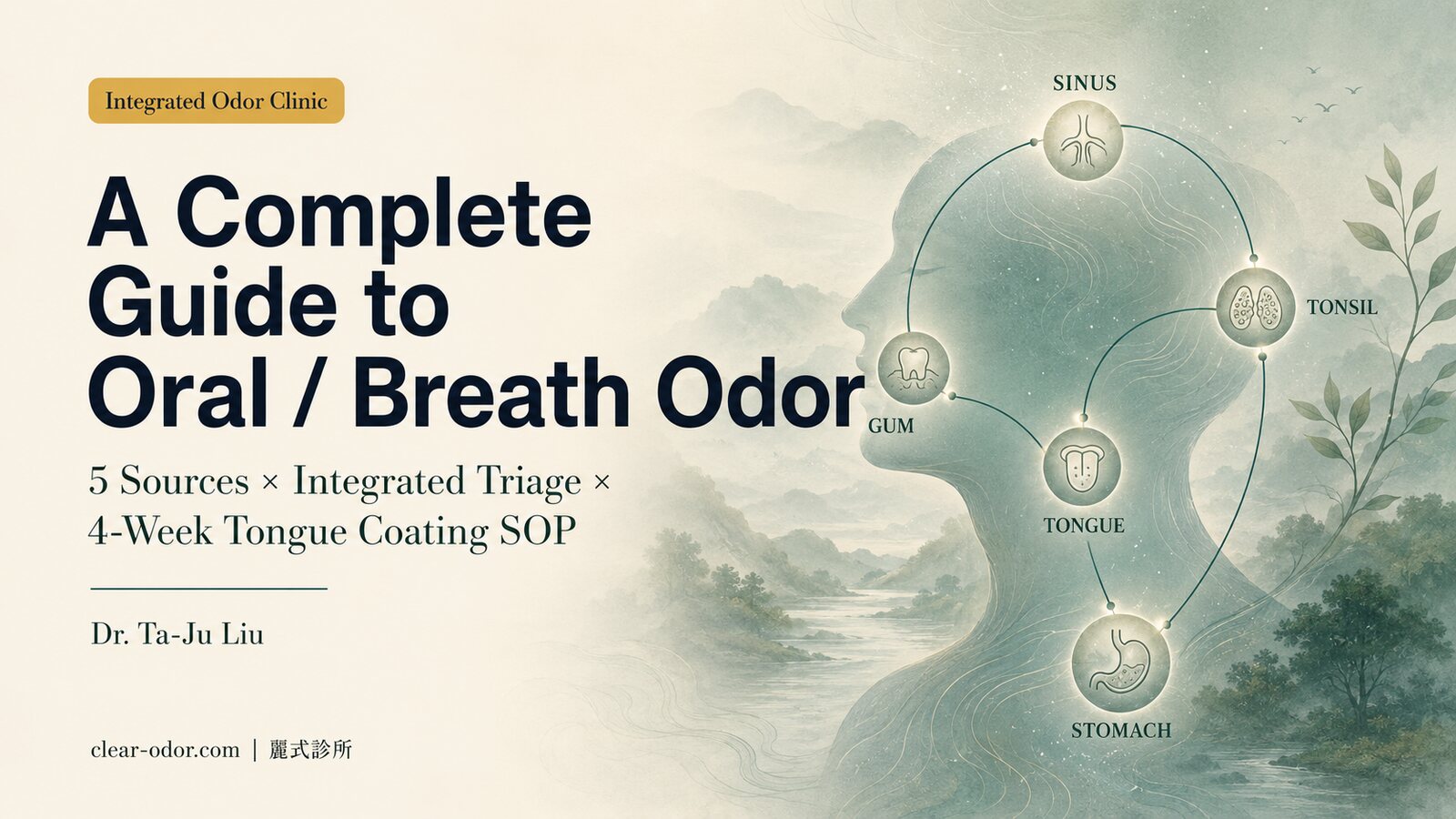
Bad breath that won't brush away — where is it actually trapped? The five oral sources
The biggest is the tongue coating on the back of the tongue, followed by periodontal disease, tonsil stones, post-nasal drip, and midlife dry mouth — and they all share one thing: they're in a toothbrush's blind spots.The five sources at a glance
The vast majority of bad breath that won't brush away comes from the five sources below. They have one thing in common — they're all in a toothbrush's blind spots. Read this table first and you'll likely be able to identify which one your smell most resembles:
| Source | Where it gets trapped | Odor / clues | Why brushing can't reach it | First-line management |
|---|---|---|---|---|
| Tongue coating (the biggest) | The back third of the dorsum of the tongue | Persistent, worst on waking, putrid | Brushing only cleans the teeth, not the back of the tongue | Mechanical debridement with a tongue scraper |
| Periodontal disease / dental plaque | Tooth gaps, gum sulcus, deep in periodontal pockets | Putrid, often with bleeding gums | Brush and floss can't reach the bottom of the pocket | Scaling, periodontal treatment |
| Tonsilloliths (tonsil stones) | Tonsil crypts | Strongly putrid, coughed up as white-yellow lumps | Deep in the throat, brushing can't touch them | ENT irrigation and assessment |
| Post-nasal drip / sinusitis | The back wall of the throat | Phlegmy smell, with nasal congestion and a runny nose | The source is in the nasopharynx, not the front of the mouth | ENT |
| Midlife dry mouth | The whole mouth | Breath worse on waking and in the afternoon | Insufficient saliva, bacteria proliferate across the board | Hydration, medication review |
Now let's go through these five one at a time.
The five sources, one by one
Tongue coating — the number-one hotbed of bad breath. The back of the tongue, especially the back third near the throat, has countless tiny papillae on its surface that form natural low-oxygen grooves — the ideal breeding ground for anaerobic bacteria and VSCs. Most people only ever brush their teeth and never clean the tongue their whole lives, which is the number-one reason for "bad breath that brushing won't get rid of." A thick white or thick yellow tongue coating is often the main source of the smell. Periodontal disease / dental plaque — hiding where the brush can't go. Plaque and tartar build up in the gum sulcus and periodontal pockets, where anaerobic bacteria continuously produce odor while also causing inflamed, bleeding gums. Once a periodontal pocket deepens, the cleaning reach of a brush and floss can't get to the bottom — which is why people with periodontal problems still have strong breath no matter how diligently they brush. Tonsilloliths (tonsillolith) — the culprit most easily overlooked. The surface of the tonsils has many recessed crypts where shed cells, food debris, bacteria, and the calcium in saliva accumulate day after day, forming rice-grain-sized, white-yellow, soft-tofu-textured calcified lumps. They give off an extremely strong putrid smell, and brushing won't clean them off at all (they're not on the teeth to begin with). Many people don't know they have them until, during a cough or while clearing the throat, they cough up an unbelievably foul white-yellow lump and suddenly understand. Post-nasal drip / chronic sinusitis — the smell flows down from above. Secretions from the sinuses or nasal cavity drip backward to the back of the throat, and this protein-containing mucus likewise gets broken down by bacteria to produce odor. The smell often carries a hint of phlegm or pus and comes with clues like nasal congestion, a runny nose, and throat-clearing. Brushing can't reach this kind of source because it isn't in the front of the mouth at all. Midlife dry mouth — the amplifier that makes the other four worse. Saliva flushes away food residue and has an antibacterial action — it's the mouth's natural cleaning system. After midlife, saliva production naturally declines, and many chronic-disease medications (blood-pressure drugs, antihistamines, antidepressants, diuretics, and so on) make the mouth even drier, with polypharmacy adding insult to injury — the less saliva there is, the more easily all the anaerobic bacteria proliferate. This is also why morning breath is especially strong: during sleep, saliva production drops to its lowest, and bacteria work unrestrained all night long. For a complete breakdown and triage of the sources of bad breath, see Bad Breath Brushing Won't Fix? 5 Sources & Which Doctor.Key takeaway: Among the five major oral sources, the biggest is the tongue coating on the back of the tongue, followed by periodontal disease, tonsilloliths, and post-nasal drip. What they have in common is that "they're all in a toothbrush's blind spots" — which is the real reason "I try so hard to brush and it does nothing."
Why do I still have bad breath after brushing and using mouthwash?
It isn't a lack of effort — the source sits beyond a toothbrush's physical reach: the biofilm on the back of the tongue, periodontal pockets, tonsil crypts, and the deep cavities of wisdom teeth and decay, where bristles simply can't go.A lot of people are stuck on one instinct: if there's a smell, you haven't brushed enough. So they brush harder, brush longer, switch to more expensive toothpaste — and the frustration only deepens. The problem isn't the level of effort; it's the physical limits of a toothbrush. Let's lay out the places it can't reach:
The four blind spots a toothbrush can't reach
Tongue coating needs "scraping," not "brushing." The anaerobic bacteria on the back of the tongue aren't dust floating on the surface — they're a colony adhering as a layer of biofilm. The chemical ingredients in toothpaste can mask it at most; what actually works is mechanical debridement — using a tongue scraper to gently scrape a few times from the base toward the tip of the tongue, physically removing that layer of bacterial film. Brushing your teeth without cleaning the tongue is like cleaning your room every day but never touching the dirtiest carpet. Tooth gaps and periodontal pockets — the bristles simply can't get in. The spaces between teeth, inside the gum sulcus, and at the bottom of deepened periodontal pockets are sealed spaces the bristles can't reach. This is why floss, interdental brushes, and regular scaling matter so much — they deal precisely with the toothbrush's blind spots. Tonsil crypts are deep in the throat. Tonsil stones get trapped in the recessed crypts of the tonsils, at the very back of the mouth near the throat, where brushing can't even touch them. Picking at them yourself with a cotton swab risks injury and gagging; the safer approach is to ask an ENT specialist to assess and irrigate them. Wisdom teeth and the deep cavities of decay are filth-trapping blind spots. Crooked or partially impacted wisdom teeth often create crevices a brush can't reach; deep cavities from decay likewise trap food residue and breed anaerobic bacteria. These structural blind spots can't be cleaned out by brushing and need dental treatment.Switching direction beats brushing harder
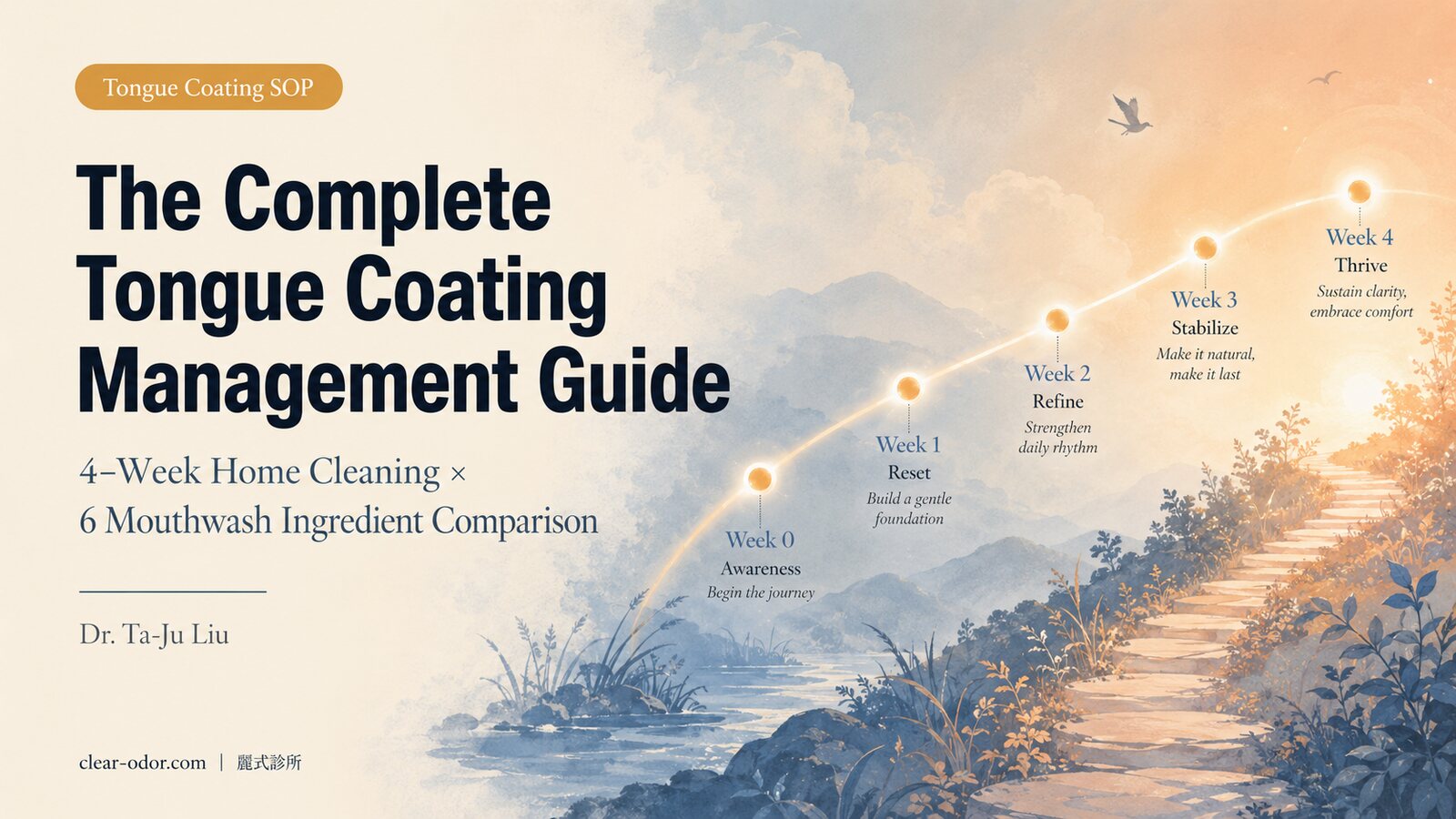
In other words — "brushing won't get rid of it" isn't a lack of effort; it's that the source of the smell is where a toothbrush can't reach. Switching direction (cleaning the tongue, flossing, scaling, dealing with the tonsils and deep cavities) is often far more effective than brushing harder. The correct method and frequency for cleaning tongue coating are laid out in Tongue Coating & Bad Breath: A 4-Week Cleaning Guide.
Can GERD cause bad breath?
It can, but it's only one of many non-oral sources and shouldn't be the first one blamed — without reflux clues like acid regurgitation and heartburn, don't pin the blame on the stomach first.At this point, someone will surely want to ask: "What about my GERD (gastroesophageal reflux disease)? My endoscopy really did show reflux."
Let's be clear: GERD can indeed be one source of bad breath, but it shouldn't be the first one blamed. This is the biggest and most stubborn myth about bad breath — "bad breath means a bad stomach."
Why "the smell of the stomach rising up" doesn't hold
Why does this instinct not actually hold up? Medical reference sources (such as the MSD Manual) clearly state that GI disease is in fact rarely a typical cause of bad breath. The key lies in the anatomy: when you're not swallowing and not refluxing, the esophagus is collapsed and closed — it's not a tube that's constantly open to air, so the smell in the stomach doesn't usually drift up to the mouth in a steady stream. So the picture of "the smell of the stomach rising all the way up to cause bad breath" doesn't match real physiology.
When GERD really is relevant, these reflux clues show up
So when is GERD genuinely related to bad breath? The answer is — when you also have other clues of reflux at the same time. If your bad breath comes with these symptoms, the stomach is worth considering:
- Acid regurgitation, often having sour or bitter fluid in the mouth
- Heartburn (a burning sensation in the chest and upper abdomen)
- Regurgitation after lying down, waking at night choking on acid
- Chronic cough, a lump-in-the-throat feeling, hoarseness (reflux irritating the throat)
Key takeaway: "Bad breath = bad stomach" is the biggest myth. When there are no clues like acid regurgitation, heartburn, or nighttime regurgitation, you shouldn't blame the stomach first. Cleaning up the mouth (tongue coating, periodontal disease, tonsils) first is the more efficient order — and the one that better fits the medical evidence.
Dr. Ta-Ju Liu says:
In clinic, I've seen far too many people take stomach medication for the better part of a year because of bad breath, with no reduction in the smell at all. Every time I hear "but I've been taking stomach medication for so long," I feel a little sad for them — it's not that the medication doesn't work, it's that the direction was wrong from the start. Stomach medication acts on the stomach, but the odor factory is in the mouth.
My habit is to walk the patient through the sources in order: see whether there's a thick layer of coating on the back of the tongue, whether there's a periodontal problem, whether it might actually be tonsil stones. Once these stages are cleaned up, many people's bad breath improves markedly. Only after the mouth has been thoroughly checked, and when there genuinely is acid regurgitation and heartburn, do I ask gastroenterology to help evaluate the reflux.
Treating bad breath as a "source problem" rather than a "stomach problem" is often the key to saving yourself half a year of going down the wrong road. If you're stuck in this struggle, you can briefly describe the situation when booking, and during the consultation we'll sort out the source together.
Which doctor should I see for bad breath, and when is the problem beyond the mouth?
The order is dentist first, then ENT, then internal medicine; only look beyond the mouth to the whole body when it persists after a thorough oral check and the odor is distinctive with whole-body symptoms. An integrated odor clinic can help sort out the source.The vast majority of bad breath comes from the oral sources discussed above, but a small group of people genuinely have bad breath caused by a problem further upstream in the body.
Four signals to look beyond the mouth
The four conditions below are signals for judging "you should look beyond the mouth / to the whole body" — the more of them you meet, the more worthwhile it is to widen the scope of investigation:
- It persists even after the mouth has been thoroughly dealt with: you've had scaling and periodontal treatment, cleaned the tongue coating diligently for a while, had the tonsils checked, and the smell is still there.
- The odor pattern is very "distinctive" and out of proportion to hygiene: not the ordinary putrid smell, but a strange odor like fruity, ammonia (urine-like), fishy, or sweet-musty.
- The smell is present in the breath, sweat, and urine all at once: the source isn't only in the mouth but is given off through multiple channels across the whole body — this usually points to metabolism inside the body, not a local oral problem.
- It comes with whole-body symptoms: excessive thirst and urination, unexplained weight loss, jaundice, persistent fatigue, altered consciousness, and so on.
The order to see doctors: dentist first, then ENT, then internal medicine
When you meet these conditions, seeing doctors in the following order is more efficient than a scattershot approach:
| Step | Specialty | When to go | What it handles |
|---|---|---|---|
| First | Dentist | The first stop for almost all bad breath | Scaling, tongue-coating assessment, periodontal disease, wisdom teeth / decay, a preliminary look at the tonsils; the highest-value first step |
| Second | ENT (otolaryngology) | When it persists after the dentist, or comes with nasal congestion, runny nose, tonsil stones, chronic sinusitis, or post-nasal drip | Upper-airway and nasopharyngeal sources |
| Third | Internal medicine / metabolic medicine | When it persists after both mouth and ENT, or the odor is distinctive (fruity, ammonia, fishy) with whole-body symptoms | Ruling out whole-body metabolic disease; for a suspected emergency (fruity breath + excessive thirst and urination, altered consciousness) go straight to the ER |
If you also have odor trouble in other locations (underarms, scalp, feet) and aren't sure where to start, you can first use the odor map for a preliminary location-by-location triage to find the main source that most needs to be addressed first. How to identify these distinctive metabolic-type odors and how to refer them is collected in Whole-Body Metabolic Odor: TMAU, Diabetes & Liver Signals; if your bad breath appears together with body odor that got stronger after midlife, you can also see Showers Daily but Still Smells? Midlife Odor: Which Doctor?.
It's worth adding that bad breath may have more than one source — it's not rare for tongue coating, periodontal disease, and tonsil stones to coexist, and for the approach to handling these multiple coexisting sources, see When Bad Breath Has Many Sources: Gums, Sinus & GERD.
Common Q&A
Q1. I brush my teeth very thoroughly every day — why do I still have bad breath?
Because the source of the smell very likely isn't on the teeth. The most common is the tongue coating on the back third of the tongue, followed by tooth gaps and periodontal pockets and the tonsil crypts — all blind spots a toothbrush can't reach. "Brushing thoroughly" and "having bad breath" can hold true at the same time, because the place you brush (the teeth) and the place producing the odor (the back of the tongue, the periodontium, the tonsils) aren't the same spot. Clean the tongue, floss, and get regular scaling first, and it often improves by more than half.
Q2. Which doctor should I see for bad breath?
Generally, it's advised to see a dentist first to address the largest oral source of bad breath (scaling, tongue coating, periodontal disease, a preliminary look at the tonsils). If it persists after the dentist has checked, or comes with symptoms like nasal congestion and a runny nose, then see ENT. Only when both the mouth and ENT have been checked and it still persists, or the smell is very distinctive (fruity, ammonia, fishy) and comes with whole-body symptoms, do you go to internal medicine / metabolic medicine to rule out whole-body disease.
Q3. Is bad breath really not a stomach problem? I've been taking stomach medication for a long time.
The vast majority of bad breath isn't a stomach problem. Medical sources note that GI disease is rarely a typical cause of bad breath, because the esophagus is normally collapsed and closed, so the smell in the stomach doesn't usually drift up in a steady stream. GERD is just one of the many non-oral sources of bad breath, and it usually comes with clues like acid regurgitation, heartburn, and nighttime regurgitation. If you don't have these symptoms, taking stomach medication alone is unlikely to solve bad breath — you should go back and check the mouth thoroughly first.
Q4. When I smell my breath right after brushing it seems fine — does that mean I don't actually have bad breath?
Not necessarily reliable. Right after brushing, with toothpaste used, the mint smell will cover it up for a short while; add olfactory fatigue, and the person themselves is inherently the least able to smell their own breath. A more reliable way to judge is to consider the consistent reactions of the people around you, or to get an objective oral assessment in an unbrushed state, rather than concluding from "I can't smell it myself."
Q5. When I cough, I cough up a small white-yellow thing that smells terrible — what is that?
That's very likely a tonsil stone — a calcified lump formed over time from bacteria, food debris, and calcium in the tonsil crypts, with a soft-tofu texture, an extremely foul smell, and impossible to clean off by brushing. It's a commonly overlooked source of bad breath. Picking at it yourself risks injury and gagging; if it recurs or the smell bothers you, it's advisable to ask an ENT specialist to assess and irrigate it.
Q6. Why is morning breath especially strong?
Because saliva production drops to its lowest during sleep. Saliva has a flushing and antibacterial action — it's the mouth's natural cleaning system; when saliva drops during sleep, anaerobic bacteria break down protein residue and produce VSCs unrestrained all night, so breath is strongest when you wake up. Saliva already decreases after midlife, and many chronic-disease medications make the mouth even drier, so strong morning breath becomes more pronounced. Cleaning thoroughly before bed and hydrating regularly during the day will help.
Q7. Mouthwash and chewing gum only last a little while — what should I do?
Because mouthwash and gum deal with the "odor," not the "source." They can temporarily mask or dilute it, but they don't remove the bacterial film on the back of the tongue, don't clean out the bacteria in the periodontal pockets, and don't deal with tonsil stones, so the effect can only last for a while. What's truly effective is mechanical debridement targeting the source — cleaning the tongue, flossing, scaling, and dealing with the tonsils and deep cavities when needed. Masking only treats the symptom; clearing out the source is the real cure.
Bad breath can, in most cases, be traced and dealt with
Bad breath and oral discomfort can, in most cases, "be traced and dealt with." Our integrated team means both the in-mouth and outside-the-mouth sources of bad breath can be assessed and handled in-house: family physician Dr. Yen-An Lin focuses on burning mouth syndrome, bad breath, and oral health (in-mouth and metabolic sources); ENT specialist Dr. Wan-Chun Tsai (with a focus on oral conditions and aesthetic medicine) can assess outside-the-mouth sources such as the sinuses, post-nasal drip, and tonsil stones. Only when the issue is confirmed to be a dental structural problem (decay, periodontal treatment needed) do we help arrange a referral to dentistry. Sort out the source first, rather than rushing to blame the stomach.
If you've been bothered by long-standing bad breath or oral discomfort, you're welcome to book an assessment.
Related Reading
- Bad Breath Brushing Won't Fix? 5 Sources & Which Doctor
- Tongue Coating & Bad Breath: A 4-Week Cleaning Guide
- Others Say You Smell but You Can't? Real vs Pseudo Odor
- When Bad Breath Has Many Sources: Gums, Sinus & GERD
- Sudden Strange Body Odor or Breath? 5 Disease Red Flags
- Oral / Halitosis Integrated Triage
- Midlife Body Odor & Aging Odor Guide
Final Thoughts
"Bad breath that won't brush away" is a struggle far too often mistaken for "a bad stomach" when it's actually "the wrong source." It leaves the person frustrated — they try so hard to brush, and it does no good at all — and leads many to gradually give up after "taking stomach medication for half a year with no effect."
The position of the odor-integration clinic is simple: this smell is real, it deserves to be taken seriously, and in most cases the source can be found and dealt with step by step. Rather than brushing furiously or taking stomach medication endlessly, it's better to first check the tongue coating, periodontal disease, and tonsils in the mouth one at a time and point the way — self-care where self-care is due, referral to dentistry or ENT where referral is due, and for the few who should look to the whole body, we'll discuss the referral path together.
Finally, please be sure to remember this safety reminder: if your bad breath comes with a fruity, ammonia, fishy, or sweet-musty smell, or together with unexplained rapid weight loss, excessive thirst and urination, jaundice, or altered consciousness — don't stop at the level of mouthwash or supplements; please see a doctor first to rule out whole-body disease; a fruity smell on the breath combined with excessive thirst and urination — go straight to the ER. These are the few, but once they're in play and get delayed, the cost is high, so it's worth 30 seconds to cross-check.
If you or a family member are stuck with bad breath, you're welcome to find Dr. Ta-Ju Liu and book a consultation, and during the consultation we'll sort out the source together.