
Why Your Antiperspirant Probably Isn't Failing You — You're Just Using the Wrong One, the Wrong Way
In clinic, the single most common sentence I hear is: "Doctor, I've tried every brand. Nothing works."
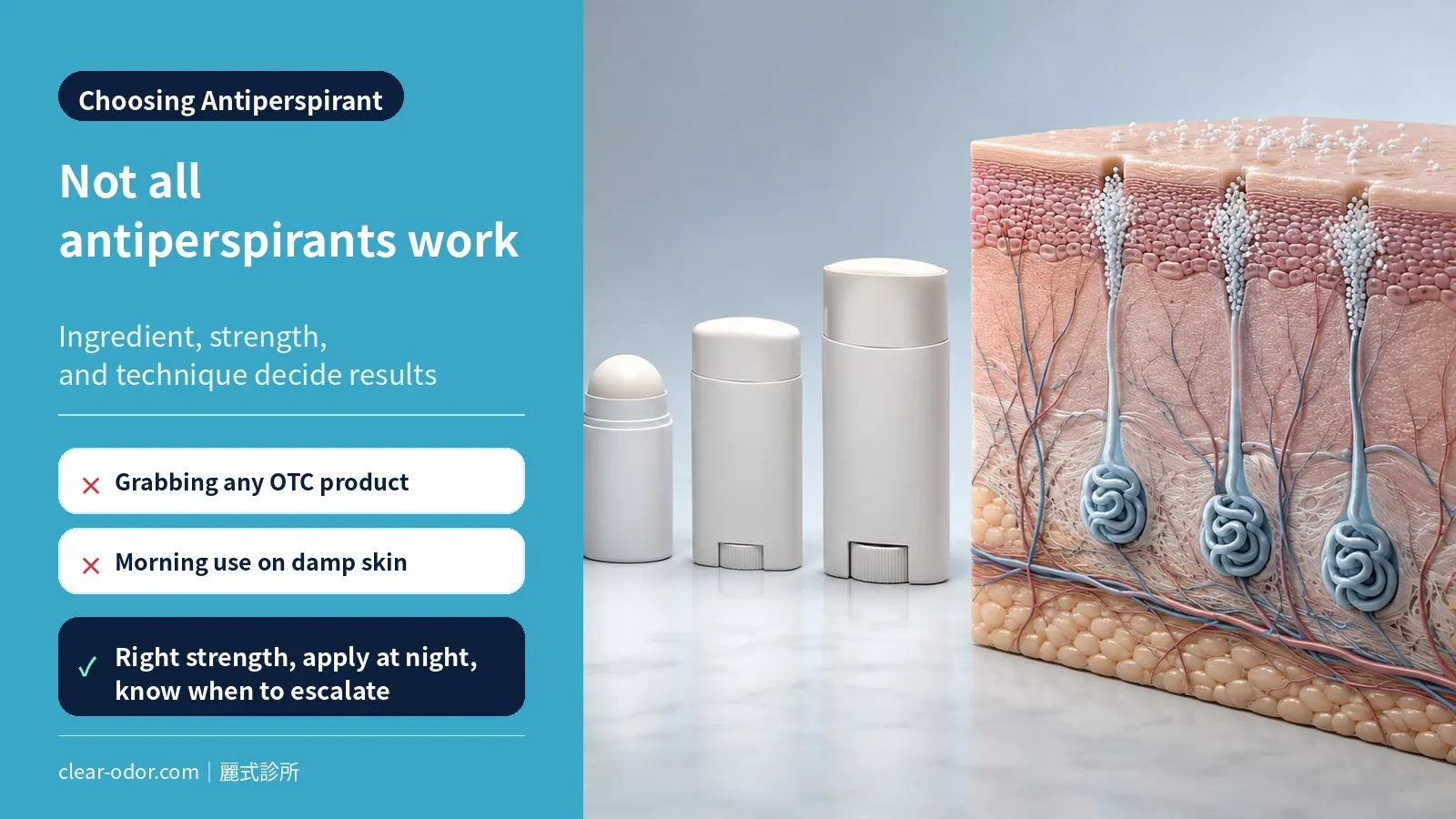
When I dig deeper, the issue is rarely a uniquely stubborn case. It's almost always one of two things: the wrong active ingredient and strength, or the wrong application technique. The gap between a drugstore deodorant stick and a properly applied 20% aluminum chloride solution like Driclor is roughly an order of magnitude. And the same tube of Driclor, applied at 7 a.m. before work, performs nothing like it does applied at 11 p.m. before bed.
Antiperspirants are the first rung of the entire sweat and odor ladder — and the cheapest one. Used correctly, they keep around 70% of moderate cases comfortable without ever needing botulinum toxin or surgery. Only after you've hit the ceiling of correct use does it make clinical sense to escalate.
In this guide I'll walk you through the decision framework I use in my own practice: ingredient differences, strength tiers, the night-application protocol that most patients miss, when to stop pushing antiperspirants and consider the next step, and the safety questions that come up over and over (aluminum and breast cancer, aluminum and Alzheimer's — what the evidence actually says).
What ingredient actually makes an antiperspirant work?
Almost every effective antiperspirant relies on an aluminum salt — aluminum ions react with sweat to form a temporary "plug" at the duct opening. The only differences are the form of aluminum, the concentration, and the strength of that plug, which is what decides the tier you need.Virtually every effective antiperspirant relies on an aluminum salt. The differences come down to which salt, what concentration, and how aggressively it plugs the sweat duct.
| Ingredient | Typical concentration | Strength tier | Common products |
|---|---|---|---|
| Aluminum chloride hexahydrate | 12–25% | Prescription / strongest | Driclor, Hyperdri, Anhydrol Forte |
| Aluminum zirconium tetrachlorohydrex GLY | 15–25% | Mid-strong (clinical OTC) | Most "Clinical Strength" sticks |
| Aluminum chlorohydrate | 15–25% | Mild (daily OTC) | Most everyday roll-ons |
| Aluminum sesquichlorohydrate | ~25% | Mid | Several European brands |
How they actually work
The mechanism is mechanical: aluminum ions react with sweat inside the eccrine duct, forming an insoluble aluminum-protein plug that physically blocks sweat release. The plug lasts roughly several days to one or two weeks before it sloughs off with natural skin turnover, which is why reapplication is needed.
A critical distinction: antiperspirants reduce sweat, not odor. If your problem is smell rather than wetness, the rest of this guide will explain why you may need a different pathway entirely.How are antiperspirant strengths tiered, and where should you start?
Clinically there are three tiers: drugstore basics (low), cosmetic "clinical strength" (medium), and prescription-grade high-concentration aluminum chloride (high, e.g. Driclor 20%). Start at the lowest strength that controls your symptoms and step up only if needed — not max strength from day one.Clinically, I sort antiperspirants into three tiers:
Tier 1: Daily / Mild OTC (aluminum chlorohydrate 15–20%)
For Grade 1 mild sweating — noticeable only with exercise, heat, or nerves; no visible stains on most clothing. Standard daily roll-ons sit here. Morning application is fine.
Tier 2: Clinical Strength OTC (aluminum zirconium 15–25%)
For Grade 1–2 moderate sweating — visible stains, daily concern, salt rings on dark synthetic fabrics. Mitchum Clinical, Secret Clinical Strength, Dove Clinical sit here. Apply at night for best results.
Tier 3: Prescription Strength (aluminum chloride hexahydrate 12–25%, e.g., Driclor 20%)
For Grade 2–3 moderate-to-severe sweating — through-shirt wetness, social avoidance, sweat-pad dependence. Driclor 20% and Hyperdri are the standards. Strict nighttime application + morning wash-off is mandatory or skin irritation becomes the dominant problem.
💡 Clinical note: If you're already on a Clinical Strength stick and reapplying twice daily without satisfaction, the answer is not "more" — it's either stepping up to prescription strength or moving on to botulinum toxin / surgical options. Individual results may vary.
How are you actually supposed to apply it, and why do 90% get it wrong?
The key is "apply at night, wash off in the morning": put it on completely dry underarms before bed (not while sweating, not right after a shower), let the aluminum form its plug overnight, then rinse in the morning — the same bottle of Driclor can work an order of magnitude better when applied correctly.This is the section worth slowing down for. The same bottle of Driclor performs an order of magnitude better when applied correctly.
Rule 1: Apply to completely dry skin
Out of the shower, skin still damp? Wrong. Aluminum salts react with surface water before they ever reach the duct opening, and you'll sting. Wait at least 30 minutes after showering, then blot the underarm dry with tissue before application.
Rule 2: Apply at night, not in the morning
This is the most counterintuitive and most important rule.
Eccrine sweat glands are at their lowest output during sleep. A nighttime application gives the aluminum salt 6–8 hours in a low-sweat, undisturbed environment to react with the duct walls and build a stable plug. A morning application is the opposite — you apply, walk into the heat, sweat washes it away before any plug forms, and you've effectively done nothing.
Rule 3: Rinse off in the morning
Rinse the underarm with plain water (no soap needed) when you wake up. The plug has already formed inside the duct; rinsing only removes surface residue. This dramatically reduces fabric staining and daytime irritation without affecting efficacy.
Rule 4: Loading phase, then maintenance
| Phase | Frequency | Duration |
|---|---|---|
| Loading | Every night | 3–7 consecutive nights |
| Maintenance | 1–2 nights per week | Long-term |
| If efficacy fades | 2–3 nights in a row, then return to maintenance | — |
Most people try it for two days, see no result, and quit. The plug takes 3–7 nights to fully establish. Give it a week.
Rule 5: Don't apply on freshly shaved skin
Microabrasions from shaving + acidic aluminum chloride = guaranteed sting and redness. Wait at least 24 hours after shaving. Shave on a day when you don't plan to apply that night.
When should you stop relying on antiperspirants alone?
When you're already using the highest tolerable strength correctly and still can't control it, when your skin is repeatedly irritated, or when odor (B.O.) bothers you more than sweat — antiperspirants target sweat, and they hit a ceiling against the odor that apocrine glands produce.Antiperspirants are excellent but they have a ceiling. Here are the four signals that you've reached it:
1. Six months of correct use without satisfaction
This is the reasonable upper bound of conservative therapy. If you've stepped up to prescription strength, applied at night, run a proper loading + maintenance phase, and still can't reach a comfortable quality of life — pushing further is not going to help. Time to evaluate botulinum toxin injection or rotational shaver minimally invasive surgery.
2. Persistent skin irritation that won't resolve
Redness, itching, peeling, or burning lasting more than two weeks despite lowering concentration and frequency means your skin doesn't tolerate aluminum salts well. Continuing only causes chronic inflammation and hyperpigmentation. Stop and evaluate alternatives.
3. Odor — not wetness — is your real problem
This is the most commonly confused point.
Antiperspirants reduce eccrine sweat. They do not address apocrine secretions. Bromhidrosis odor comes from apocrine gland secretions being broken down by skin bacteria — a process largely independent of eccrine sweat. If your complaint is "I smell even when I'm dry" or "I smell in winter when I don't sweat," even the strongest antiperspirant can only help indirectly (by keeping skin drier and reducing bacterial activity). It can't address the source.For this scenario, see → Bromhidrosis Guide: Causes, Diagnosis, Treatment & Recovery, and the decision framework in Underarm Odor: Antiperspirant vs Botox vs Surgery.
4. Daily quality of life is suffering
Antiperspirants are a daily chore — remember to apply, carry a stick for touch-ups, worry about whether tonight's protocol will hold tomorrow. If that anxiety has become a meaningful drag on your social or professional life, the math often favors one-and-done minimally invasive surgery over indefinite daily management.
Do antiperspirants have side effects? Can they harm skin, cause cancer or dementia?
By far the most common side effect of antiperspirants is local skin irritation: stinging, redness, dryness, or itching, usually reversible and closely tied to concentration and technique (skipping night application, applying to damp or freshly shaved skin); as for the circulating claims of "cancer, dementia, or trapping toxins inside the body," the current evidence does not support them. Separating what genuinely warrants attention (skin irritation) from what's been exaggerated (systemic harm) keeps you from abandoning a first-line tool that is safe and effective for most people just because of internet rumors.The genuinely common side effect: local skin irritation
High-concentration aluminum chloride (such as Driclor 20%) is acidic as it forms the plug at the sweat-duct opening, so it can irritate the skin. Most stinging, redness, and peeling isn't actually "an allergy" but a technique problem: applying to skin that isn't dry, applying in the daytime (where sweat washes it away), applying the same night you shaved, or jumping concentration too fast. Following the earlier rules — night application, fully dry skin, 24 hours after shaving — reduces most irritation substantially. If you truly can't tolerate it, lower the concentration or evaluate other treatments rather than pushing through to chronic inflammation.
What you're allergic to is often the "fragrance," not the aluminum salt
Many people assume that reacting to an antiperspirant means an aluminum allergy. In fact, the more common culprit of contact dermatitis is the fragrance and preservatives in the product, not the active aluminum salt itself. If one product itches and switching to a fragrance-free formula fixes it, the fragrance was likely the problem. Choosing a fragrance-free formula — or asking a doctor for a fragrance-free prescription antiperspirant — is often more practical than abandoning antiperspirants altogether.
"If the sweat can't get out, won't it poison me or cause heatstroke?"
It won't "poison" you, but spraying it all over isn't necessary either. An antiperspirant only blocks the local eccrine sweat-duct openings where it's applied (mainly the underarm), which is a tiny fraction of all the body's sweat glands; the rest of your body still sweats and dissipates heat normally, so blocking the underarm does not "trap toxins inside." Conversely, there's no need to spray antiperspirant over large areas of the body — broadly sealing off sweating doesn't help heat dissipation and is especially unnecessary in hot weather or heavy exercise. Just treat the areas that actually bother you."Aluminum causes cancer and dementia"? The current evidence doesn't support it
"Aluminum-salt antiperspirants cause breast cancer / cause Alzheimer's" are the two most widely circulated concerns, but so far, epidemiological and clinical research has not confirmed these causal links, and the WHO, the American Cancer Society, and the FDA do not endorse them. The evidence details for these two are laid out in the next section, "Common Myths."
Can I use it during pregnancy or breastfeeding?
Standard-concentration antiperspirants are considered acceptable during pregnancy and breastfeeding; if you still have concerns, you can choose a low-concentration, fragrance-free formula, or discuss it with a doctor case by case. At any stage, if you develop a persistent skin reaction out of proportion to the antiperspirant, stop using it and have a doctor evaluate — don't keep cycling through brands on your own.
Key takeaway: What matters with antiperspirants is "skin irritation" — a real, controllable, local issue — not the systemic fears amplified online. With the right concentration, a fragrance-free formula, and night application, the vast majority of people can use them safely long-term; and if one truly doesn't suit you, evaluating botox or minimally invasive options is always still on the table.
What are the common antiperspirant myths worth clearing up?
The four most-asked myths — does aluminum cause breast cancer, does it cause Alzheimer's, are aluminum-free "natural" deodorants healthier, and is more product better — are each checked against the current evidence here; the takeaway is that the right ingredient, strength, and technique matter far more than switching brands.Myth 1: "Aluminum causes breast cancer"
This claim traces to a 2003 speculative paper. No epidemiological or clinical study since has confirmed an association between aluminum-based antiperspirants and breast cancer. The WHO, American Cancer Society, and FDA all reject this link.
Myth 2: "Aluminum causes Alzheimer's disease"
The hypothesis dates to the 1970s–80s but larger subsequent studies have not confirmed a causal relationship between antiperspirant use and dementia. The WHO's 2017 dementia risk review did not include aluminum-based antiperspirants as a risk factor.
Myth 3: "Natural / aluminum-free deodorants are healthier"
"Aluminum-free deodorants" do not reduce sweat at all — they only mask odor with fragrance or inhibit bacteria with baking soda or alcohol. If your goal is "don't sweat," aluminum-free products are guaranteed to fail. For purely odor-driven users with mild cases, they may suffice; for moderate-to-severe bromhidrosis, they generally don't.
Myth 4: "More is better"
False. The reactive sites at the duct opening are finite. Excess aluminum just sits on the skin surface causing irritation without strengthening the plug. Thin, nightly, consistent beats thick layers every time.
Frequently Asked Questions
Q1: Does night vs morning application really matter that much?
A1: Yes, dramatically. Prescription-strength products like Driclor only deliver their full effect when applied at night. Mild OTC products tolerate morning application reasonably well, but even they perform better with nighttime use. Individual results may vary, but clinical satisfaction is consistently higher in the nighttime group.Q2: Can baking soda replace antiperspirant?
A2: No. Baking soda transiently buffers skin pH and inhibits bacteria — it does not reduce sweat. It's a natural deodorant, not an antiperspirant, and the two are not interchangeable.Q3: What age can children use antiperspirant?
A3: Mild OTC products are generally fine from about age 12. Prescription-strength products such as Driclor should wait until at least age 16 and ideally be evaluated by a dermatologist to avoid prolonged irritation on developing skin.Q4: What about sensitive skin?
A4: Start with the lowest reasonable concentration (aluminum chlorohydrate 15%), shorten contact time (apply at bedtime, rinse if you wake at night), and consider a thin layer of 1% hydrocortisone as a barrier before application. If irritation persists, botulinum toxin injection skips the skin contact problem entirely.Q5: What if I have redness and stinging after shaving?
A5: Pause antiperspirant for 24–48 hours and use a fragrance-free moisturizer to restore the skin barrier. Schedule shaving for a day when you don't need to apply that night — for example, shave Saturday, apply Sunday night.Q6: When should I actually see a doctor?
A6: Book an evaluation if any of these apply:- One month of correct Driclor use without satisfaction
- Recurrent skin irritation you can't tolerate
- Sweating that interferes with sleep, work, writing, or driving
- Odor — not wetness — is your primary concern
- You want to understand botulinum toxin or minimally invasive surgery options
Q7: What are the side effects of antiperspirants? Is long-term use safe?
A7: The most common side effect is local skin irritation (stinging, redness, itching), usually tied to technique or concentration and reversible; contact dermatitis from fragrance is more common than from the aluminum salt itself, and switching to a fragrance-free formula often helps. "Cancer, dementia, trapping toxins inside" are not supported by current evidence. An antiperspirant only blocks local underarm sweat glands and doesn't impair whole-body heat dissipation, but there's also no need to spray it over large areas. If a persistent skin reaction out of proportion to the antiperspirant appears, stop and have a doctor evaluate.Antiperspirant Decision Flow
How severe is your underarm sweating?- Mild (occasional) → OTC mild (chlorohydrate), morning application
- Moderate+ (daily concern) → Clinical Strength or prescription Driclor → Strict night apply + morning rinse, 7-night loading phase → Reassess at 1 month
- Satisfied → Maintenance 1–2/week
- Not satisfied / irritation → Evaluate escalation
- Botulinum toxin (4–6 mo cycles)
- Minimally invasive surgery (long-term)
Related Reading
- Bromhidrosis Guide: Causes, Diagnosis, Treatment & Recovery
- Underarm Odor: Antiperspirant vs Botox vs Surgery
- Sweating by Area: Palms, Underarms & Feet Treatment
- Axillary Bromhidrosis
- Hyperhidrosis & Compensatory Sweating
Conclusion: Push Antiperspirants to Their Ceiling, Then Decide
Antiperspirants are the base of the entire sweat and odor pyramid — inexpensive, reversible, available anytime. Before considering anything more aggressive, I want every patient to first use them correctly: pick the right tier, apply at night, run the loading and maintenance phases, and reassess at six months.
If you've done that and you're still not where you want to be, you now have a very strong case to escalate. Botulinum toxin buys 4–6 months of dry, sweat-free comfort. Rotational shaver surgery addresses the apocrine glands directly for long-term improvement in both odor and sweat. Individual results may vary, but logically: antiperspirant is the foundation, not the ceiling.
Related Reading
- Bromhidrosis Guide: Causes, Diagnosis, Treatment & Recovery
- Underarm Odor: Antiperspirant vs Botox vs Surgery
- Sweating by Area: Palms, Underarms & Feet Treatment
- Axillary Bromhidrosis
- Hyperhidrosis & Compensatory Sweating
About Clear Odor Clinic
Dr. Ta-Ju Liu, Director, Clear Odor Clinic- Areas of focus: minimally invasive surgery for axillary, areolar, and groin bromhidrosis; hyperhidrosis treatment
- Signature technique: rotational shaver apocrine gland clearance — 4 mm incision, complete apocrine gland clearance as the goal
- Clinical experience:
- 20+ years specializing in odor and sweat treatment
- 10,000+ documented surgical cases
- Board-certified dermatologist (Taiwan)
- Philosophy: "Antiperspirants are a great tool but not a magic one. Using them correctly is step one. Knowing when to stop and escalate is step two — and both of those decisions are something we can sort out together in clinic."