
Sweaty Palms Are Not Simply About "Being Nervous"
Many people with sweaty palms have been misled their whole lives by one sentence: "You're just too nervous."
That sentence is only half true. Nervousness does worsen palm sweat — but a true hyperhidrosis patient has wet palms even when they are not nervous, not hot, sitting quietly. It is not an emotional problem; it is a medical condition with a clear pathological mechanism, one that can be classified by type and graded by severity.
Working out "which type and which grade you are" is the starting point for everything that follows — because primary and secondary hyperhidrosis call for completely different treatment directions, and a mild case calls for a different strategy than a severe one. This article exists to make those two things clear.
Primary vs Secondary Hyperhidrosis: Sort These Two Out First
Sweaty palms (a form of hyperhidrosis) are clinically divided into two major categories. This is the most important first cut.
| Comparison | Primary hyperhidrosis | Secondary hyperhidrosis |
|---|---|---|
| Cause | Constitutional — overactive sympathetic nerve signalling | Caused by another condition or medication |
| Sweating area | Focal, symmetric (both hands, sometimes with feet, underarms) | Often generalised, or asymmetric |
| When it occurs | When awake; usually stops once asleep | May also occur during sleep |
| Age of onset | Usually childhood or adolescence | Often appears in adulthood |
| Family history | Common | Less consistent |
| Underlying cause | None — the sweat glands themselves are normal | Thyroid overactivity, endocrine imbalance, infection, medication, menopause, etc. |
Key point: Distinguishing primary from secondary is not an academic detail — it is the first step that bears on safety. If secondary sweating (caused, for example, by a thyroid problem) is treated as plain hyperhidrosis, the real disease is missed.
Why Does Primary Hyperhidrosis Happen? A Sympathetic-Nerve "Signal Overload"
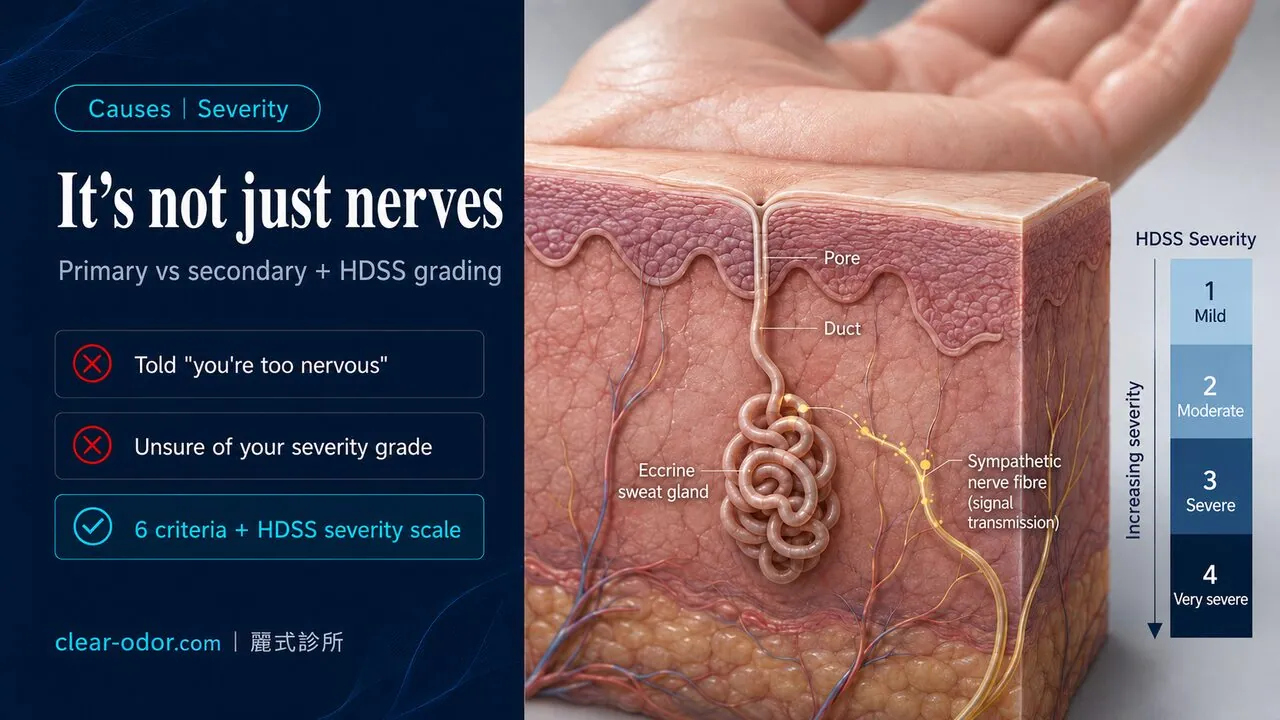
To understand primary hyperhidrosis, start with one fact: the number and structure of the sweat glands (eccrine glands) on your hands are no different from anyone else's.
The problem is not the glands, but "the nerve that directs the glands." Sweat secretion is controlled by the sympathetic nervous system, which issues a "sweat" command when the body needs to shed heat or is under stress. In primary hyperhidrosis, this nerve's signalling is abnormally active and its threshold is set low, so the palm's sweat glands keep being driven even in situations where most people would not sweat.
This also explains several of hyperhidrosis's typical features:
- It usually stops after falling asleep: because sympathetic activity drops during sleep
- Emotion and stress make it worse: because emotion further stimulates the sympathetic nerve
- Palms and soles are especially affected: the sweat glands here are naturally more influenced by emotional sweating
It is worth emphasising: primary hyperhidrosis is a benign constitutional condition — not an organ failure, and it does not "deteriorate into some disease." What it affects is quality of life and social confidence, not lifespan or health — and for patients long troubled by it, that is often important reassurance.
Is Hyperhidrosis Hereditary?
Yes. Primary hyperhidrosis has a clear tendency to cluster in families. Clinically, a high proportion of patients, when asked, have a parent, sibling or other relative with the same trouble; the inheritance pattern is thought to carry an autosomal dominant tendency.
But "having a family history" should be understood correctly on two counts:
- An inherited trait does not mean equal severity. Within the same family, some are severe and some only mildly affected — the variation is wide.
- A family history actually aids diagnosis. Family history is one of the diagnostic criteria below; it makes the "primary" classification clearer.
If a child at home has had persistently wet palms from a young age that affect writing or making friends, an in-person assessment by a doctor is advised. Management in children must consider age and development, and the timing of assessment can be discussed with the doctor.
Do You Have Hyperhidrosis? 6 Diagnostic Criteria
Clinically, a widely used set of criteria is used to judge "primary focal hyperhidrosis." First, one prerequisite must be met:
Focal, visible, excessive sweating, lasting at least 6 months, with no obvious cause found.
Given that prerequisite, look at the following 6 items. Meeting at least 2 of them strongly supports a diagnosis of primary hyperhidrosis:
- The sweating areas are bilateral and symmetric
- The sweating impairs daily life or work
- It occurs at least once a week
- It began before age 25
- There is a family history
- Sweating stops once asleep
If you would like a more lifestyle-oriented first check, you can also use the Hyperhidrosis Severity Self-Check: 5 Quick Questions — that article uses 5 yes/no questions to help you decide whether to manage it through lifestyle measures or seek a clinic assessment.
Severity Grading: How to Tell Mild, Moderate and Severe Apart
Once hyperhidrosis is confirmed, the next question is "how severe." Clinically, the HDSS (Hyperhidrosis Disease Severity Scale) is commonly used, matching your situation to a single sentence:
| Grade | Description | Severity |
|---|---|---|
| HDSS 1 | My sweating is never noticeable and never interferes with daily activities | Minimal |
| HDSS 2 | My sweating is tolerable but sometimes interferes with daily activities | Mild–moderate |
| HDSS 3 | My sweating is barely tolerable and frequently interferes with daily activities | Severe |
| HDSS 4 | My sweating is intolerable and always interferes with daily activities | Severe |
The reading logic is simple: HDSS 1–2 leans toward conservative management first; HDSS 3–4 clearly calls for active treatment. The scale's focus is not the objective millilitres of "how much sweat," but "whether the sweat is hindering your life" — which is exactly the core criterion for whether hyperhidrosis should be treated.
Key point: Hyperhidrosis is not a question of "whether you sweat," but of "whether the sweat hinders your life." An HDSS 3 patient may not produce the most sweat in the room, yet already dare not shake hands, dare not handle paper documents, and have touchscreens fail constantly — that life-level interference is the signal for active treatment.
At HDSS 3–4, options on the treatment ladder include Iontophoresis for Sweaty Palms: Devices, Frequency, Results, botulinum toxin injection and newer topical drugs; a full comparison is in Sweaty Palms: 3 FDA-Approved Non-Surgical Treatments.
When Should You Suspect "Secondary" Hyperhidrosis?
Although most hyperhidrosis is primary, a few signals that "do not look like typical primary" should prompt you to rule out secondary hyperhidrosis first:
- It started suddenly in adulthood (primary usually appears in childhood or adolescence)
- Generalised heavy sweating, not confined to the palms
- Marked sweating during sleep too (night sweats)
- One-sided, asymmetric sweating
- Accompanied by other symptoms such as weight change, palpitations, fever, fatigue
If any of the above appear, it should not be treated directly as plain hyperhidrosis — a doctor should first clarify the underlying cause, which may involve thyroid, endocrine, infectious or medication factors. Confirm the cause first, so the treatment direction does not go astray.
Which Specialty Should You See for Hyperhidrosis?
For a first-line assessment of hyperhidrosis, starting with dermatology is advised. A dermatologist can help you:
- Confirm whether it is primary or secondary, arranging tests to rule out underlying disease if needed
- Assess HDSS severity
- Plan the treatment ladder by severity (from topical antiperspirants and iontophoresis to injections)
If, after assessment, a surgical option is considered, a referral to the relevant specialty follows. The key point is: you do not need to jump straight to thinking about surgery. With a correct classification and grading first, most patients can find an acceptable option at a non-surgical stage.
Frequently Asked Questions
Q1: Only my hands sweat — not my feet or underarms. Is that still hyperhidrosis?
Yes. Primary hyperhidrosis can present in a single area. Affecting only the palms still meets the diagnosis; whether the soles or underarms are also involved varies from person to person.
Q2: Will hyperhidrosis go away on its own?
Primary hyperhidrosis is constitutional and usually does not disappear on its own. Some people see a slight decrease in sweat volume in adulthood, but for most it persists. It does not "deteriorate into a disease," but it rarely "cures itself" either.
Q3: Is hyperhidrosis the same as "sweating easily"?
No. It is normal for anyone to sweat in heat, during exercise, or when nervous — that is thermoregulation. Hyperhidrosis is when the palms stay wet enough to affect life even when it is not hot, you are not active, and you are not nervous.
Q4: My hand sweat increased only in adulthood — is that a concern?
It is worth noting. Onset only in adulthood, or accompanied by generalised sweating, night sweats or weight change, looks less like typical primary hyperhidrosis — seeing a doctor first to rule out secondary causes is advised.
Q5: Does hyperhidrosis have to be treated?
Not necessarily. HDSS 1–2 with no clear life impact can first be observed and managed conservatively. HDSS 3–4 that already hinders work and social life is best actively addressed. The decision rests on "how much the sweat interferes with your life."
Related Reading
- Iontophoresis for Sweaty Palms: Devices, Frequency, Results
- Hyperhidrosis Severity Self-Check: 5 Quick Questions
- Sweaty Palms: 3 FDA-Approved Non-Surgical Treatments
- Palmar Hyperhidrosis
- Hyperhidrosis & Compensatory Sweating
Conclusion
Hyperhidrosis is not "being too nervous" — it is a medical condition that can be classified and graded. The correct order for addressing it is: first separate primary from secondary → confirm the diagnosis with the 6 criteria → grade severity with HDSS → plan the treatment ladder by grade.
The great majority of hyperhidrosis is a benign primary constitution, affecting quality of life rather than health; but a minority of secondary cases may hide another disease behind them, so "atypical" signals must always be ruled out first.
Dr. Ta-Ju Liu has 20 years of experience in odor and sweat treatment, offering classification assessment, severity interpretation and treatment-ladder planning for hyperhidrosis. If you are unsure which type or grade your hand sweat is, you are welcome to book a consultation for an in-person assessment by the doctor. You can also explore the full treatment options of the palmar hyperhidrosis specialist service.
Related Reading
- Iontophoresis for Sweaty Palms: Devices, Frequency, Results
- Hyperhidrosis Severity Self-Check: 5 Quick Questions
- Sweaty Palms: 3 FDA-Approved Non-Surgical Treatments
- Palmar Hyperhidrosis
- Hyperhidrosis & Compensatory Sweating
This article is for health education. Individual results may vary. The classification, severity and treatment direction of hyperhidrosis must be confirmed after an in-person assessment by Dr. Ta-Ju Liu.