Why Another Hyperhidrosis Guide?
Hyperhidrosis is one of the most persistently misunderstood medical conditions I see in clinic.
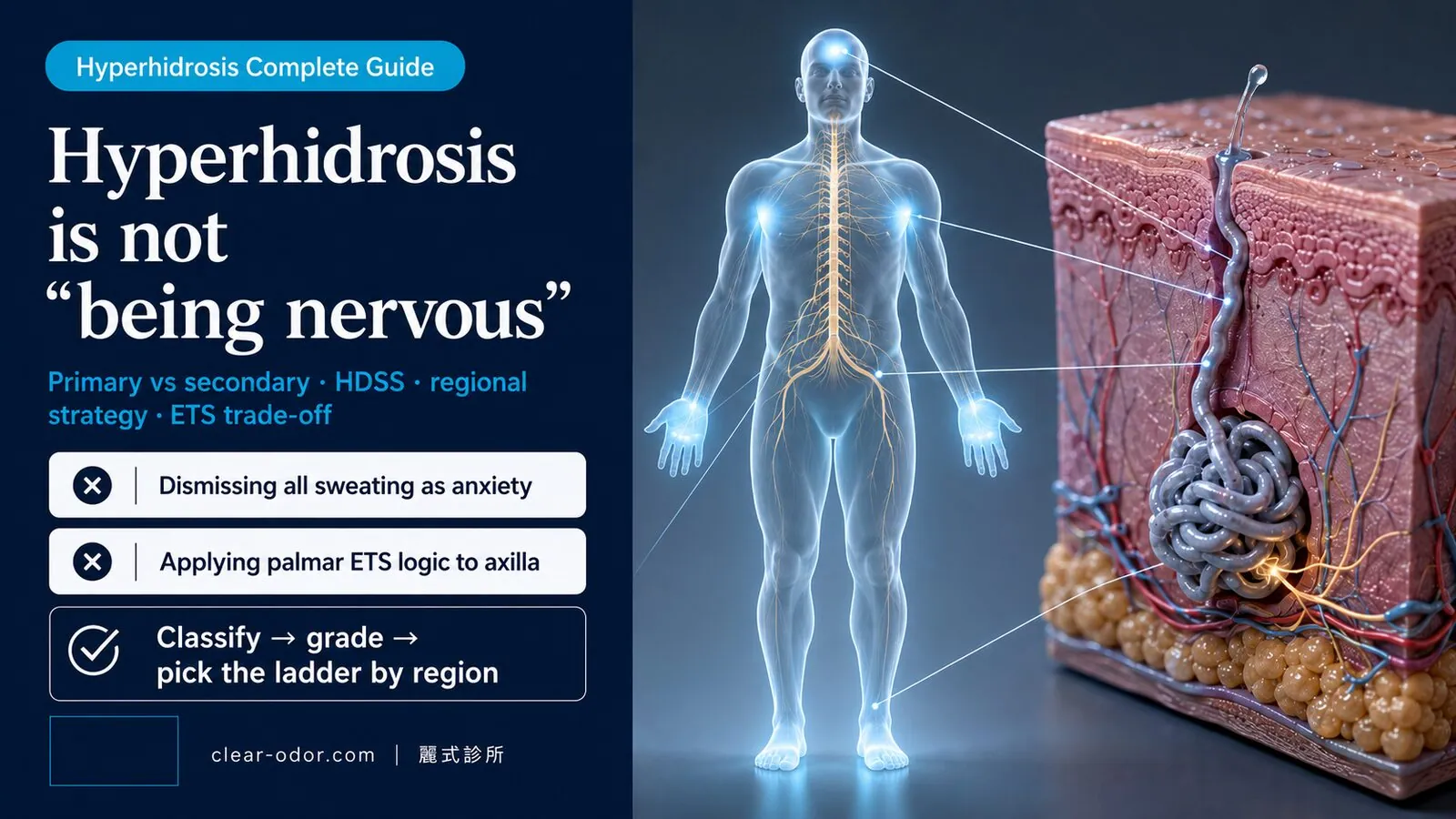
The single phrase patients hear most often, going back to childhood, is "you're just nervous." It only captures half the picture. People with true hyperhidrosis sweat heavily even when they're calm, cool, and sitting still — because the underlying problem is not emotion. It's a constitutional condition with a clear pathophysiologic mechanism, a recognized diagnostic standard, and a structured treatment ladder.
In 20 years of clinical practice, the most common pattern I see is not severity — it's uncertainty. Patients don't know whether their case is primary or secondary, don't know which HDSS grade warrants active treatment, don't know whether to start with antiperspirant or iontophoresis, don't know why some surgeons recommend ETS while others strongly counsel against it.
This guide consolidates the questions I get asked most often into one path: differential diagnosis → self-grading → body region differences → treatment ladder → the ETS trade-off → managing compensatory hyperhidrosis → decision framework. By the end you should be able to answer:
- Is my hyperhidrosis primary or secondary? Do I need to rule out other conditions first?
- Which HDSS grade am I? Should I be actively seeking treatment?
- Is the treatment strategy the same for palmar, axillary, and plantar sweating?
- Why do some patients regret ETS? What exactly is compensatory hyperhidrosis?
- I already had ETS — are there non-nerve-cutting options for the compensatory sweating I now have?
Individual outcomes vary. This guide provides a decision framework, not a diagnosis. The final treatment choice still requires in-person evaluation.
Multi-site odor? Start with the map, then the self-check. If you have odor in more than one area, see the Odor Map for site-by-site triage first, then run the Self-Assessment to score severity — usually faster than booking a single specialty up front.
What is hyperhidrosis, and is the cause really not "being nervous"?
Hyperhidrosis is defined as sweating beyond what's needed to regulate temperature — sweating per se isn't hyperhidrosis. It's mainly driven by overactive sympathetic nerve signals and has no necessary link to "being nervous"; anxiety can worsen it but isn't the root cause.The medical definition of hyperhidrosis is: sweat output exceeding what the body needs for thermoregulation. Sweating during heat, exercise, or stress is normal. Hyperhidrosis refers to sustained sweat gland activation in situations that don't call for cooling.
To understand the condition, start with one important fact:
The sweat glands of a hyperhidrosis patient are structurally normal. The problem isn't the glands — it's the nerve signal driving them.Eccrine sweat glands are controlled by the sympathetic nervous system. When the body needs to dissipate heat, or when it's under stress, sympathetic nerves fire and trigger sweating. In primary hyperhidrosis, the threshold is set abnormally low and the signal is abnormally active — so the glands fire continuously in conditions that wouldn't trigger most people.
This mechanism explains several typical features of primary hyperhidrosis:
- Stops during sleep — sympathetic activity naturally falls during deep sleep
- Worsens with emotion and stress — sympathetic nerves respond strongly to emotional input
- Concentrated at palms, soles, and axillae — these are the regions most heavily innervated for emotion-driven sweating
A reassurance point worth emphasizing: primary hyperhidrosis is a benign constitutional state, not a sign of organ dysfunction, and it does not "progress into another disease." It affects quality of life and social confidence — not lifespan or general health. For patients who have lived with the burden for years, this is often the single most important thing to hear.
Why Is Hyperhidrosis Genetic?
Primary hyperhidrosis shows a clear familial clustering pattern — a substantial proportion of patients have a parent, sibling, or other first-degree relative with the same condition. The inheritance pattern is generally considered autosomal dominant with variable penetrance.
But "having a family history" should be interpreted carefully:
- Genetic predisposition doesn't dictate severity — within the same family, some members are severely affected, others only mildly. Phenotypic variability is wide.
- Family history aids diagnosis — it's one of the 6 diagnostic criteria below, and helps support a primary diagnosis.
When Does Hyperhidrosis Begin? When Does It Ease?
Primary hyperhidrosis typically appears in childhood or adolescence, peaks in symptom severity from the 20s through 40s, and may mild down somewhat after age 40 — but it does not "spontaneously resolve," because the underlying sympathetic hyperactivity is constitutional.
If your sweating started suddenly in adulthood, that's an important red flag for ruling out secondary causes (hyperthyroidism, endocrine disorders, infection, etc.) — covered in detail in Section 11.
Why must you first split hyperhidrosis into "primary" and "secondary"?
Because their treatments differ entirely: primary is focal, symmetric, with no other cause, and you treat the symptom itself; secondary is whole-body sweating caused by a disease or medication, where you treat that underlying cause first — mistaking secondary for primary misses the real disease.The first step in evaluating any hyperhidrosis case is always to distinguish primary from secondary — because the treatment direction is entirely different, and treating secondary hyperhidrosis as primary means missing the underlying disease.
| Comparison | Primary Hyperhidrosis | Secondary Hyperhidrosis |
|---|---|---|
| Cause | Constitutional — overactive sympathetic signaling | Caused by another disease, medication, or hormonal change |
| Distribution | Localized, symmetric (palms, axillae, soles — typically bilateral) | Often generalized, or asymmetric |
| Timing | Daytime when awake; typically stops during sleep | May continue during sleep (night sweats) |
| Age of onset | Childhood or adolescence | Typically adult onset |
| Family history | Common | Less consistent |
| Common underlying causes | None — glands and endocrine status are normal | Hyperthyroidism, diabetes, infection (TB, other chronic), medications (antidepressants, hormones), menopause, autonomic dysfunction |
For a deeper walk-through of the primary vs secondary differential, the 6-criterion diagnostic standard, and the red-flag checklist, see Why Palms Sweat: Primary vs Secondary & a Severity Check.
Are hyperhidrosis and bromhidrosis the same problem?
No — hyperhidrosis is a "sweat volume" problem from eccrine glands, while bromhidrosis is an "odor" problem from apocrine glands plus bacteria; they often coexist and get confused, but their treatments differ (reducing sweat vs deodorizing), so sorting them out first prevents using the wrong approach."My underarm both sweats a lot and smells — are these the same problem?" This question comes up every week.
The answer: not the same problem, but commonly co-occurring. The difference comes down to two different sweat gland types:
| Comparison | Hyperhidrosis | Bromhidrosis |
|---|---|---|
| Gland source | Eccrine | Apocrine |
| Secretion | Watery, contains electrolytes | Viscous, contains protein + lipids |
| Distribution | Whole body (palms, soles, forehead, axillae focal) | Underarm, areolae, perineum, groin |
| Odor | Odorless | Has characteristic odor |
| Triggered by | Heat, emotion, spicy food | Sex hormones, emotion |
| Treatment goal | Block nerve signal to eccrine glands or destroy glands | Reduce/remove apocrine glands |
Four typical clinical patterns:
- Hyperhidrosis alone — high sweat volume, no odor → treatment targets eccrine glands (Botox, miraDry, in severe cases ETS)
- Bromhidrosis alone — distinct odor, normal sweat volume → treatment targets apocrine glands
- Combined hyperhidrosis + bromhidrosis (most common in clinic) — both gland types active → one micro rotational curettage surgery addresses both simultaneously
- Compensatory hyperhidrosis — heavy sweating on torso/back/legs after ETS sympathectomy → a separate, iatrogenic problem with a different treatment pathway (covered in Section 9)
If your primary concern is odor rather than sweat volume, start with Bromhidrosis Guide: Causes, Diagnosis, Treatment & Recovery to identify which treatment pathway applies.
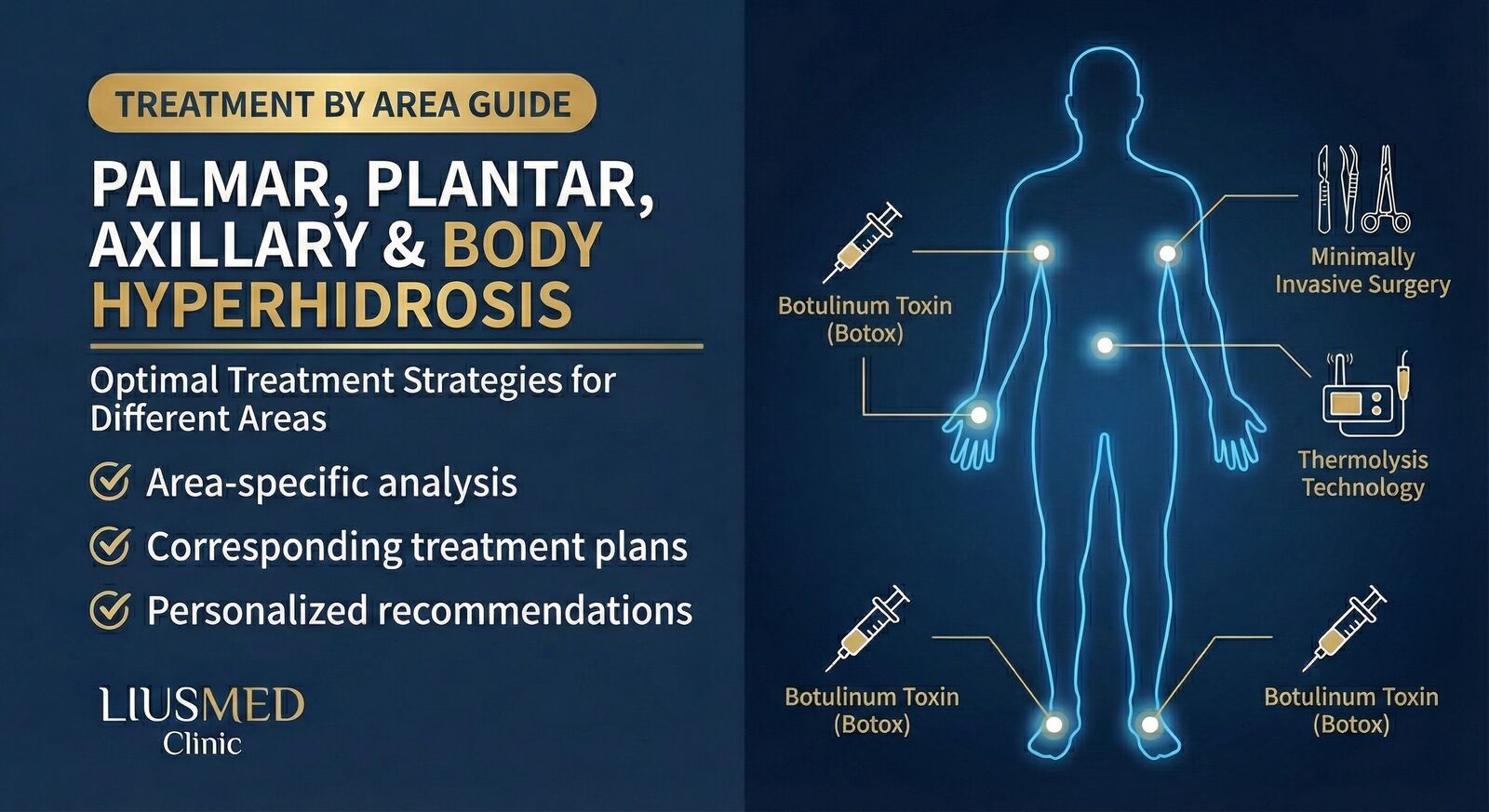
How do palmar, axillary, plantar, craniofacial, and generalized hyperhidrosis differ?
The cause may be the same (overactive sympathetic signaling), but the best treatment differs entirely: palms via iontophoresis or ETS evaluation, underarms via antiperspirant/botulinum/surgery, soles via antiperspirant and botulinum, and craniofacial and generalized have their own considerations — so the right ladder depends on the region.Hyperhidrosis is not one disease — it's a family of presentations. The mechanism may be shared (overactive sympathetic signaling), but the optimal treatment strategy differs by region. The most common patient mistake is applying "palmar hyperhidrosis logic" to axillary hyperhidrosis — and you'll see below why these two regions sit on very different paths.
a. Palmar Hyperhidrosis (Hands)
The most recognizable form. Affects roughly 3% of the population.
- Burden: writing, handshakes, touchscreen devices, precision work, certain occupations
- Treatment priority: conservative first (iontophoresis, Botox, oral anticholinergics); ETS as a last resort
- Why not start with ETS: literature reports compensatory hyperhidrosis at 20–90% incidence after thoracic sympathectomy, and the new sweating typically appears on the torso, back, and legs. Once it occurs it generally cannot be fully reversed
- Detail page: Palmar hyperhidrosis treatment
b. Axillary Hyperhidrosis (Underarms)
Affects roughly 5% of the population; frequently co-occurs with bromhidrosis (both gland types active).
- Burden: visible sweat stains on clothing, body odor, restricted wardrobe choices, social confidence
- Treatment priority: antiperspirant → Botox → micro rotational curettage (long-term for moderate-to-severe)
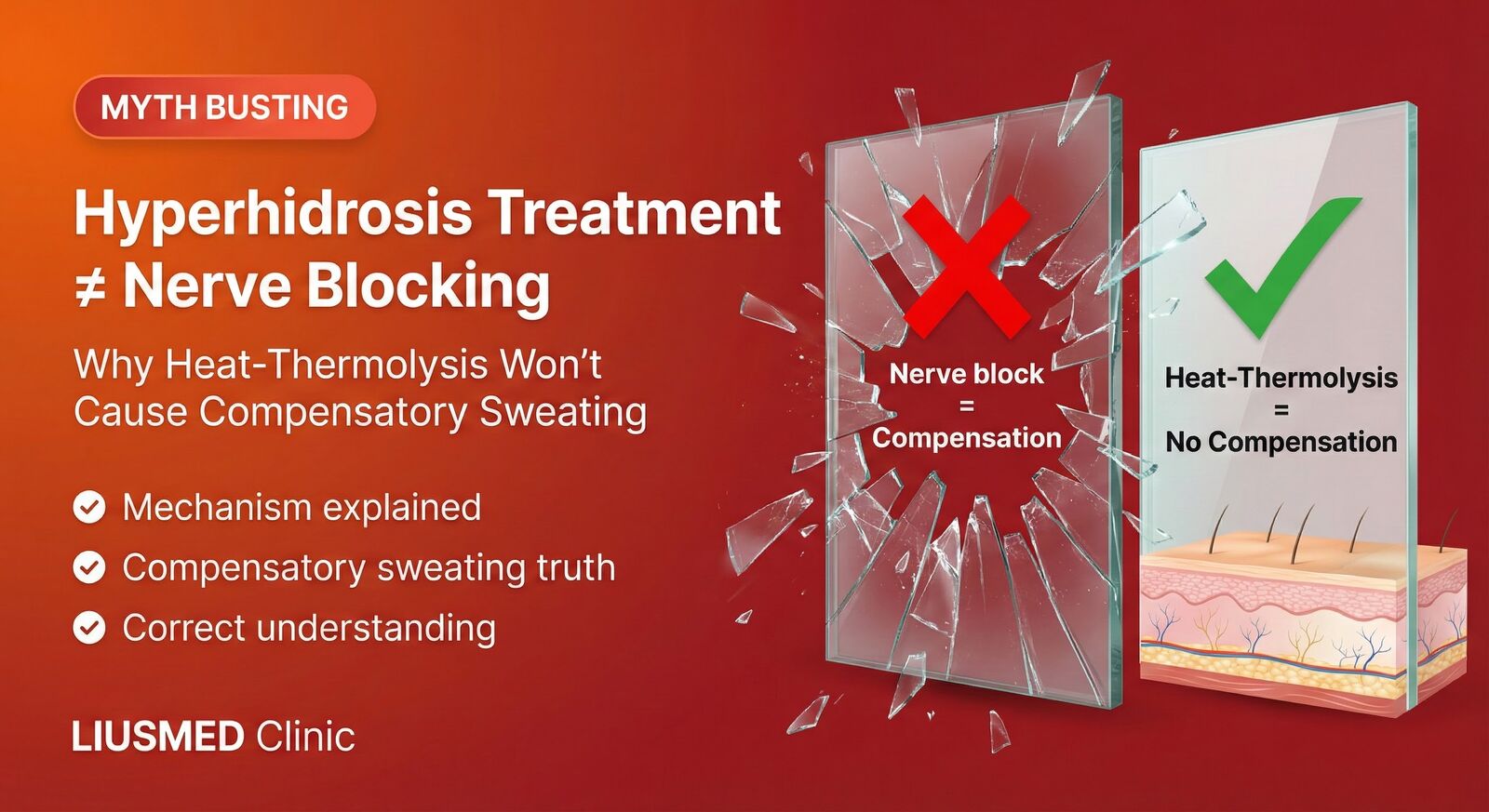
- Why axillary differs from palmar: axillary surgical options (micro rotational curettage, miraDry) do not cut sympathetic nerves — they target the sweat glands directly. No compensatory hyperhidrosis. This is the single biggest advantage of axillary hyperhidrosis treatment.
- Detail page: Axillary bromhidrosis treatment
c. Plantar Hyperhidrosis (Soles)
Affects roughly 3% of the population, often paired with foot odor (the moist environment supports bacterial and fungal growth).
- Burden: wet shoes, soaked socks, recurrent fungal infections, awkward shoe-off social situations
- Treatment priority: foot antiperspirants, iontophoresis, Botox injection
- Why no ideal surgical option: lumbar sympathectomy (for plantar hyperhidrosis) carries high compensatory risk plus risk of urogenital dysfunction — rarely performed
- Daily management: breathable footwear, change socks 1–2× daily, foot powder, rotate shoes for drying
d. Craniofacial Hyperhidrosis (Head and Face)
Affects roughly 1% of the population; highly visible in social settings.
- Burden: forehead dripping, soaked hairline, gustatory sweating (during meals)
- Treatment priority: Botox injection (forehead, hairline) — durable 4–6 months
- Why not surgery: facial ETS carries extremely high compensatory risk and can cause Horner's syndrome (ptosis, miosis, dry eye). Generally not recommended
e. Generalized Hyperhidrosis (Whole-Body)
Less than 1% of the population — but this is the category most likely to be secondary.
- Possible causes: hyperthyroidism, diabetes, tuberculosis or other chronic infection, medication side effects, autonomic dysfunction, menopause
- Approach order: workup first → treat the underlying condition if found → if truly primary after exclusion, plan symptom control
- Symptom control options: oral anticholinergics, multi-site Botox injection, lifestyle adjustments
For a comprehensive comparison of treatment strategies across all body regions, see Sweating by Area: Palms, Underarms & Feet Treatment.
How severe is your hyperhidrosis? How do you self-grade with the HDSS?
Clinicians widely use the four-level HDSS (Hyperhidrosis Disease Severity Scale): from "sweating never interferes with daily life" to "severely interferes with daily activities" — this score maps directly to whether conservative measures or active treatment fit, and it's the starting point of evaluation.Once hyperhidrosis is established, the next question is "how severe." The clinical standard is the HDSS scale (Hyperhidrosis Disease Severity Scale) — a single-sentence framework:
| Grade | Description | Severity | Recommended action |
|---|---|---|---|
| HDSS 1 | My sweating is never noticeable and never interferes with daily activities | Mild | Routine daily care suffices |
| HDSS 2 | My sweating is tolerable but sometimes interferes with daily activities | Mild-to-moderate | Antiperspirant / iontophoresis primary |
| HDSS 3 | My sweating is barely tolerable and frequently interferes with daily activities | Severe | Active treatment recommended — Botox or surgical evaluation |
| HDSS 4 | My sweating is intolerable and always interferes with daily activities | Severe | Active treatment strongly recommended |
Reading the scale is simple: HDSS 1–2 leans toward conservative management; HDSS 3–4 clearly calls for active treatment.
The Core Insight of HDSS
The scale is not asking how many milliliters of sweat you produce. It's asking whether sweat interferes with your life — and that's the right clinical question for whether to treat.
A patient at HDSS 3 may not produce the most sweat in the room, but already avoids handshakes, can't handle paper documents, has unreliable touchscreens, and brings a handkerchief to job interviews. That kind of functional interference is the signal for active treatment. Conversely, a patient who appears to sweat a lot but whose life is unaffected may not need active intervention.
For a more situational self-assessment, see Hyperhidrosis Severity Self-Check: 5 Quick Questions — five yes/no questions to determine whether you should manage at home or seek clinical evaluation.
How do you tell whether you have primary hyperhidrosis?
Clinicians use the Hornberger criteria: focal excessive sweating for at least 6 months, plus two or more of symmetric, at least weekly, onset before age 25, family history, and no sweating during sleep — while first excluding secondary causes.The clinical standard for diagnosing primary focal hyperhidrosis is the Hornberger criteria. The prerequisite:
Focal, visible, excessive sweating lasting at least 6 months, with no apparent secondary cause.
Given that, two or more of the following six criteria strongly support primary hyperhidrosis:
- Sweating is bilateral and relatively symmetric
- Sweating impairs daily activities or work
- At least one episode per week
- Onset before age 25
- Positive family history
- Sweating stops during sleep
The more criteria met, the higher the likelihood of primary hyperhidrosis. If none of the criteria fit — especially asymmetric sweating, night sweats, or adult-onset — circle back to consider secondary causes.
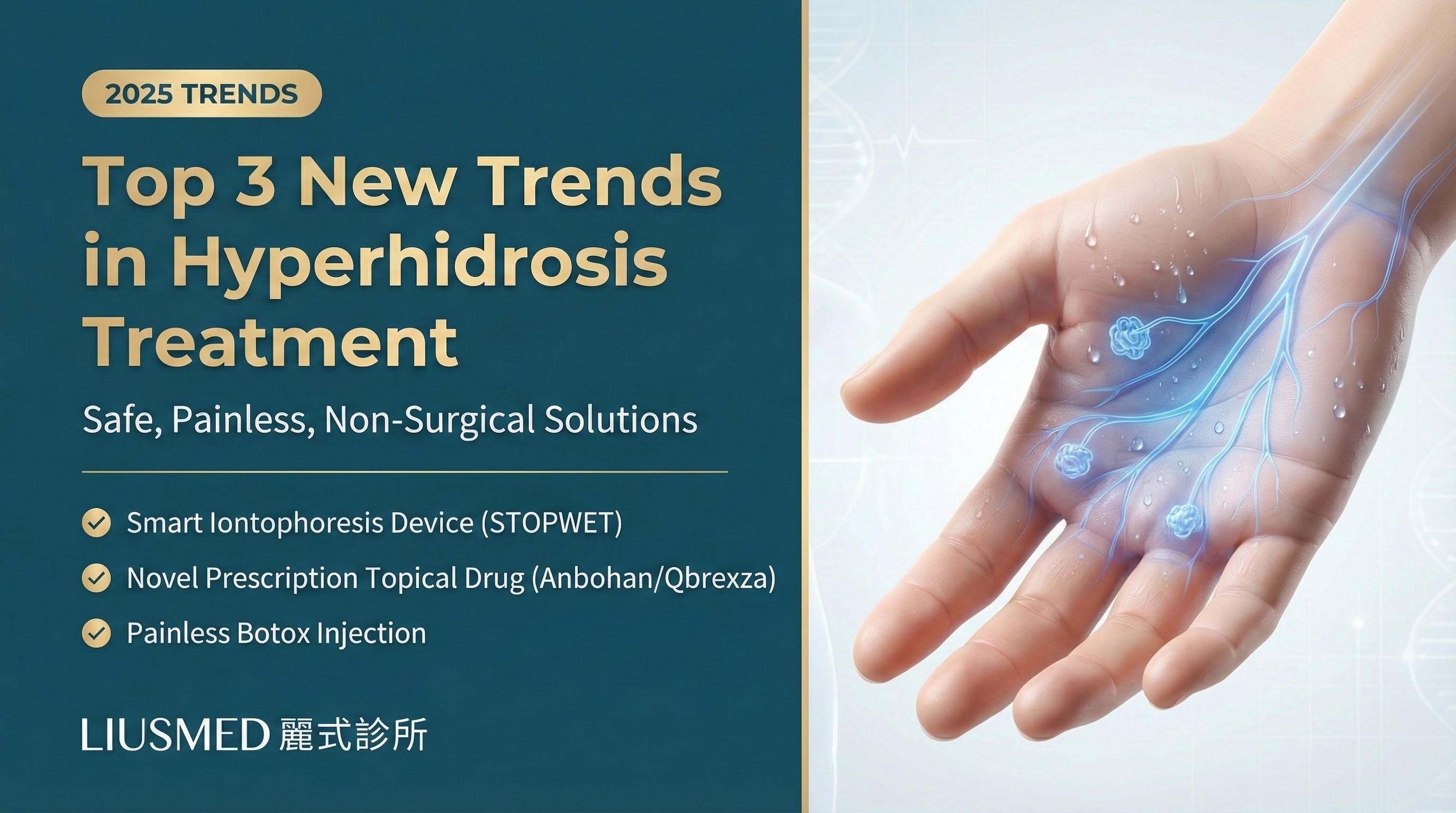
What treatment options exist, and how do you step up the ladder?
Treatment should climb a ladder, not jump straight to surgery: from conservative measures like antiperspirants and iontophoresis, to botulinum toxin, to surgery; and the best option on the ladder differs by region — push lower-invasiveness options to their ceiling first, and step up only if needed.Note: The efficacy percentages listed in each tier below are approximate ranges compiled from hyperhidrosis treatment literature; individual results vary considerably and are provided for reference only.
Hyperhidrosis treatment should not "jump straight to surgery." There's a rational ladder — escalate based on effectiveness, risk, and cost. The best option on the ladder depends on the body region.
Rung 1: Antiperspirants (HDSS 1–2)
- Aluminum chloride preparations (Driclor, ClinicalStrength) — mechanism is sweat-duct occlusion; apply at bedtime, rinse on waking
- Applicable regions: underarm, hands, feet
- Efficacy: axillary 50–70%, palmar 30–50%, plantar 40–60%
- Limitations: possible skin irritation; effect ceases when use stops; insufficient for HDSS 3–4
Rung 2: Iontophoresis (Palmar and Plantar, HDSS 2–3)
Mild electrical current passing through water reduces superficial sweat gland activity. Best suited to palms and soles.
- Protocol: initial phase 3–4× per week, 20–30 min each; maintenance 1–2× per week
- Efficacy: palmar 60–80%, plantar 60–70%
- Home use possible: with a dedicated device
- Contraindications: metal implants, pacemakers, pregnancy
- Detail: Iontophoresis for Sweaty Palms: Devices, Frequency, Results
Rung 3: Oral Anticholinergics (Generalized or Multi-Site, HDSS 2–3)
- Common drugs: glycopyrrolate (less CNS penetration, fewer central side effects), oxybutynin
- Efficacy: 50–60%
- Side effects: dry mouth, blurred vision, constipation, tachycardia — dose individualized
- Best fit: generalized hyperhidrosis, multi-region cases, patients unsuitable for local treatments
Rung 4: Botox Injection (Most Regions, HDSS 3, or Patients Avoiding Surgery)
Botox blocks the acetylcholine signal between sympathetic nerves and sweat glands — clear effect on hyperhidrosis.
- Duration per session: axillary 4–9 months, palmar 3–6 months, plantar 3–6 months
- Per-session cost: moderate, depending on region and dose
- Long-term cost: repeated 1–2× per year — the 3-year cumulative can match or exceed a one-time surgery
- Best fit: short-term need (wedding, exam), surgical contraindication or aversion, "test before committing to surgery"
Rung 5: Microwave / Radiofrequency (e.g., miraDry) — Axillary, HDSS 2–3
- Mechanism: microwave energy destroys superficial sweat glands (both eccrine and apocrine)
- Applicable region: axillae only (not suited for palms, soles, or face)
- Efficacy: 70–80% of patients maintain effect at 1 year; some report sweat return at 2–3 years
- Per-session cost: moderate-to-high
- Limitation: blind energy delivery; uniformity depends on skin thickness; deeper glands may not be fully ablated
Rung 6: Micro Rotational Curettage (Axillary, HDSS 3–4, Especially Combined with Bromhidrosis)
- Mechanism: 5–7 mm axillary incision, direct-visualization curettage of subdermal apocrine and most eccrine glands
- Efficacy: 90–95%, with < 5% recurrence at 5-year follow-up
- Simultaneously addresses bromhidrosis — best one-time treatment for combined axillary hyperhidrosis + bromhidrosis
- No sympathetic nerve cutting — no compensatory hyperhidrosis
- Detail: Axillary bromhidrosis surgical treatment
Rung 7: ETS Sympathectomy (Palmar Hyperhidrosis Last Resort — Requires Full Understanding of Compensatory Risk)
Detailed separately in the next section.
How effective is ETS sympathectomy, and how do you weigh compensatory sweating?
ETS works fast and dramatically for palmar sweating, but the trade-off is "compensatory sweating" — once the chest sympathetic nerve is cut, the body often over-sweats on the back, chest, and abdomen, and it's irreversible; so ETS is an option to weigh carefully, not decide lightly.ETS (endoscopic thoracic sympathectomy) is a thoracoscopic procedure that severs or clips the thoracic sympathetic ganglia controlling hand sweating. Palmar sweating does stop after ETS — quickly and dramatically.
The controversy isn't about effect. It's about the common side effect: compensatory hyperhidrosis.
What Is Compensatory Hyperhidrosis?
Sympathetic nerves don't only control hand sweating — they also participate in whole-body thermoregulation. When the nerve to one segment is cut, the body compensates by recruiting other regions to maintain heat dissipation. The result: previously dry areas — torso, back, abdomen, thighs — begin producing heavy sweat.
| Aspect | Detail |
|---|---|
| Incidence | Wide range in the literature, commonly cited 20–90% depending on surgical segment, cutting vs clipping, and follow-up duration |
| Common locations | Trunk, back, abdomen, thighs (large surface area) |
| Severity | Ranges from mild to severe; in some patients the compensatory sweat volume exceeds the original hand sweating |
| Reversibility | Generally cannot be fully reversed once it occurs — there's currently no reliable way to restore severed sympathetic nerves |
5 Things to Understand Before ETS
- ETS works for palmar hyperhidrosis — quickly and unambiguously. No need to doubt this.
- Compensatory hyperhidrosis is a common side effect, not a rare complication — don't only weigh "my hands will stop sweating." Weigh the compensatory risk on the same scale.
- Once it occurs, it generally cannot be fully reversed — severed sympathetic nerves can't be restored.
- This is an informed-consent decision — whether the trade-off is worthwhile is personal. Some patients are satisfied, others regret it deeply. The difference is often whether they were fully informed pre-op.
- Understand the non-nerve-cutting options first — whether you're a good candidate for ETS or another option requires individualized clinical evaluation.
For the full ETS vs hyperhidrosis differential and pre-op informed-consent essentials, see Hyperhidrosis vs Compensatory Sweating: Before ETS Surgery.
Already had ETS and stuck with compensatory sweating — is there any help?
There's a pathway that doesn't cut any more nerves — sweat-gland thermolysis: it treats the eccrine glands in the compensating area directly to reduce sweat, rather than operating again on the already-cut, irreversible sympathetic nerve; for those bothered by post-ETS compensation, it's a relatively gentle option.For patients who already had ETS and are now affected by compensatory hyperhidrosis, traditional options are extremely limited — the sympathetic nerves are already severed and cannot be restored, and another sympathectomy would only shift the compensatory pattern elsewhere.
In our clinic, this patient population is addressed with sweat gland thermolysis — a pathway that targets the sweat glands directly without touching any nerve.
Mechanism and Candidates
- Mechanism: controlled thermal energy is applied to eccrine glands at the compensatory region. No sympathetic nerve is touched at any step.
- Candidates:
- Patients with post-ETS compensatory hyperhidrosis
- Patients who are unwilling to accept ETS risk but have axillary or localized hyperhidrosis affecting daily life
- Patients with reservations about nerve-blocking treatments generally
- Why no further compensation occurs: because no nerve signal pathway is cut from start to finish, the body has no reason to "compensate" elsewhere.
Treatment Planning Considerations
Managing compensatory hyperhidrosis is highly individualized — compensation site, surface area, sweat volume, and the patient's life-priority ranking all vary. Evaluation in clinic covers:
- Documenting the specific location and extent of compensatory sweating
- The original ETS segment and timing (affects interpretation of nerve distribution)
- The patient's most-affected life situations (clothing, occupation, social context)
- Goal discussion — total sweat-volume reduction vs targeting one or two priority regions
Individual outcomes vary; feasibility and expected improvement range are confirmed in face-to-face evaluation. If you're affected by post-ETS compensatory sweating, see Hyperhidrosis and Compensatory Sweating Clinic.
Which hyperhidrosis treatment should you actually choose?
There's no single answer — decide by region, severity, the effect you want, the invasiveness and irreversible risk you'll accept (especially ETS), and your life needs; the point is to pick the option that best fits your weighting, not the most powerful one."Which treatment should I choose?" — no single answer. Decide along these dimensions:
Dimension 1: Region
Different regions sit on different optimal pathways — this is the first dimension to clarify:
| Region | First-line | Long-term option |
|---|---|---|
| Palmar | Iontophoresis / Botox / oral anticholinergic | ETS (only after full understanding of compensatory risk) |
| Axillary | Antiperspirant → Botox | Micro rotational curettage (no compensation, stable long-term) |
| Plantar | Antiperspirant / iontophoresis / Botox | No ideal surgical option — conservative-only |
| Craniofacial | Botox | Surgery not recommended (Horner risk) |
| Generalized | Rule out secondary → oral / multi-site Botox | Treat underlying condition |
Dimension 2: HDSS Severity
- HDSS 1–2: start with conservative — usually sufficient
- HDSS 3: conservative + Botox, or surgical evaluation
- HDSS 4: active treatment recommended — surgery if the region allows, otherwise long-term Botox
Dimension 3: Timeline
- Short-term (event within 6 months): Botox (effect in 4 weeks)
- Long-term: surgery (where the region allows)
Dimension 4: Cost
- Botox repeated 1–2× per year — 3-year cumulative can match or exceed a one-time surgery
- One-time surgery (axillary) — 3-year horizon: surgery is the more economical choice
Dimension 5: Surgical and Compensatory Risk Tolerance
- Can accept surgery + 7-day recovery + zero compensation (axillary): micro rotational curettage
- Can accept ETS-vs-compensation trade-off (severe palmar refractory to all else): ETS
- Cannot accept any surgery or any compensatory risk: repeated Botox + conservative
Dimension 6: Combined Bromhidrosis?
- Hyperhidrosis only, no odor: region-dependent (axillary → miraDry / micro rotational curettage; palmar → iontophoresis / Botox)
- Hyperhidrosis + bromhidrosis combined (most common at axilla): micro rotational curettage handles both in one operation
Which red flags warn that it could be "secondary" hyperhidrosis?
Several signals that aren't typical of primary: sudden onset in adulthood, whole-body rather than focal-symmetric, heavy sweating during sleep (night sweats), plus rapid weight loss, fever, or palpitations — these call for first excluding secondary causes like hyperthyroidism, infection, endocrine disease, or medication.Although most hyperhidrosis is primary, several signals are "not typical of primary" and should prompt secondary workup first:
- Adult-onset (primary typically begins in childhood or adolescence)
- Generalized whole-body sweating, not localized to palms/axillae/soles
- Night sweats during sleep
- Unilateral or asymmetric sweating
- Accompanied by weight change, palpitations, fever, fatigue
- Accompanied by neck mass, exophthalmos, arrhythmia (signs of hyperthyroidism)
- Onset after starting a new medication (antidepressants, hormones, chemotherapy)
Any of these warrants not jumping straight to hyperhidrosis treatment. Work up the underlying cause first — thyroid, diabetes, infection, medication, autonomic dysfunction, menopause are all possibilities. Get the cause right, and the treatment direction follows.
Frequently Asked Questions (FAQ)
Q1: If I have palmar hyperhidrosis and get ETS, will I definitely have compensatory sweating?
Not 100%, but the incidence is high — literature commonly cites 20–90% depending on surgical method and follow-up duration. Severity cannot be reliably predicted pre-op. Precisely because no surgeon can guarantee "you won't have it," full informed consent before ETS matters.
Q2: Does axillary micro rotational curettage cause compensatory hyperhidrosis?
No. Micro rotational curettage targets the sweat glands directly and does not cut any sympathetic nerve. The body has no reason to "compensate" elsewhere. This is the single biggest treatment advantage of axillary hyperhidrosis — and a key difference from palmar ETS.Q3: How safe is Botox for hyperhidrosis? How long does one injection last?
Botox for hyperhidrosis has a long clinical safety record. Duration: axillary 4–9 months, palmar 3–6 months, plantar 3–6 months. Most patients require 1–2 injections per year.
Q4: Can I do iontophoresis at home?
Yes — with a dedicated device. The initial protocol is more intensive (3–4× per week), maintenance is lighter (1–2× per week). Contraindicated in pregnancy, metal implants, and pacemakers. See Iontophoresis for Sweaty Palms: Devices, Frequency, Results.
Q5: I started sweating heavily as an adult — is that concerning?
Yes — worth attention. Adult-onset, generalized distribution, night sweats, or weight change collectively suggest something other than typical primary hyperhidrosis. Workup for secondary causes (thyroid, endocrine, infection, medications) should come first.
Q6: Will hyperhidrosis go away on its own?
Primary hyperhidrosis is constitutional and typically does not resolve spontaneously. Some patients see a modest reduction in sweat volume after age 40, but most continue throughout adult life. It will not "progress into a disease," but it also won't simply "cure itself."
Q7: My palms and underarms both sweat heavily — can I treat them at once?
You can treat them separately. Address the axilla first — because axillary surgery (micro rotational curettage) is a no-compensation long-term option. For the palms, start with iontophoresis or Botox (non-surgical). The two can be scheduled at different times without interaction.
Q8: How severe are the side effects of oral anticholinergics?
Common side effects include dry mouth, blurred vision, constipation, and tachycardia. Dose is individualized. Contraindicated in narrow-angle glaucoma, severe urinary retention, and myasthenia gravis. Start at a low dose and titrate to tolerance.
Q9: Does hyperhidrosis affect lifespan or general health?
No. Primary hyperhidrosis is a benign constitutional condition — it does not affect lifespan or general health. It affects quality of life and social confidence. But secondary hyperhidrosis may have an underlying cause (e.g., hyperthyroidism) that does need treatment — which is why distinguishing primary from secondary matters.
Q10: I already had ETS and now have compensatory sweating — is there anything I can do?
Yes — there are non-nerve-cutting pathways that target the sweat glands directly (see Section 9 — sweat gland thermolysis). Management of compensatory hyperhidrosis is highly individualized; feasibility and expected improvement need face-to-face evaluation. See Hyperhidrosis and Compensatory Sweating Clinic.
Q11: Can children with hyperhidrosis be treated? What age is appropriate?
Pediatric hyperhidrosis is not rare. Conservative treatments (iontophoresis, antiperspirants) can start in childhood. Any treatment involving nerve blocking or sweat gland destruction is generally deferred until development stabilizes. If you observe persistent palmar wetness affecting your child's writing or social interaction, in-clinic evaluation is appropriate.
Q12: Is hyperhidrosis treatment covered by insurance?
Coverage varies by procedure and diagnosis. In Taiwan, ETS for palmar hyperhidrosis may be covered by National Health Insurance under specific conditions, but axillary Botox, microwave, and micro rotational curettage are generally elective/out-of-pocket. Specific coverage and pricing can be confirmed with the treating physician.
When should you book a consultation?
When conservative measures are maxed out and it still bothers you, when sweating clearly affects work, social life, or mood, when you want to understand your type and full options, or when you're unsure whether it's sweating or odor — it's worth an in-person evaluation to match a plan to your region and situation.If any of the following apply, an in-person evaluation is worthwhile:
- HDSS 3 or above (sweating frequently interferes with daily activities)
- Used antiperspirant or home iontophoresis for ≥ 3–6 months with insufficient effect
- Considered Botox but tired of cumulative cost and repeat injections
- Considering ETS — want to fully understand compensatory risk and alternatives before deciding
- Already had ETS and now affected by compensatory hyperhidrosis
- "Atypical" features present (adult-onset, night sweats, asymmetric, accompanied by other symptoms) — want to rule out secondary causes first
- Combined hyperhidrosis + bromhidrosis — want both addressed at once
- Pediatric or adolescent in the family with hyperhidrosis affecting school or social life
The evaluation covers: detailed history (family history, symptom timeline, prior treatments, medications), primary vs secondary differential, HDSS grading, regional mapping, and discussion of the treatment pathway that best fits your situation.
The evaluation fee is not tied to subsequent treatment — a consult-only visit with no commitment is fine.
Closing: Returning the Decision to You
Hyperhidrosis is not "being nervous" and it's not "hopeless." It has a clear pathophysiology, a complete treatment ladder, and real choices to make based on your region, severity, and life context.
The goal of this guide is not to push you toward surgery — it's to give you an accurate framework for assessing your situation so you know which direction to step next:
- Distinguish primary from secondary first (rule out other conditions if needed)
- Use HDSS to decide whether active treatment is warranted
- Pick the right ladder for your region — palms, axillae, and soles have very different optimal paths
- ETS is not forbidden, but it should only be chosen after fully understanding the compensatory trade-off
- For those already living with compensatory hyperhidrosis, non-nerve-cutting pathways exist
If anything remains unclear after reading, you're welcome to book a one-on-one evaluation. In the clinic we walk through each option side by side.
Related Reading
- Sweating by Area: Palms, Underarms & Feet Treatment
- Hyperhidrosis vs Compensatory Sweating: Before ETS Surgery
- Hyperhidrosis Severity Self-Check: 5 Quick Questions
- Why Palms Sweat: Primary vs Secondary & a Severity Check
- Bromhidrosis Guide: Causes, Diagnosis, Treatment & Recovery
- Hyperhidrosis & Compensatory Sweating
- Palmar Hyperhidrosis
- Axillary Bromhidrosis
- Body Odor & Hyperhidrosis Conditions