
Why Understand the Apocrine Gland Before Deciding on Treatment?
Every week in clinic, patients arrive with variations of the same questions:
- "I've had body odor since middle school — is this a disease?"
- "Why do antiperspirants stop the sweat but not the smell?"
- "My father doesn't have body odor, but my grandmother does — is this genetic?"
- "My friend says her odor faded after age 50. Will mine?"
The answer to all of these points to a single organ: the apocrine gland (also called the large sweat gland or apocrine sweat gland).
The apocrine gland isn't a "broken sweat gland" or an "abnormal tissue" — it's a normal part of human physiology, evolutionarily preserved for pheromone signaling and social communication. It's modern society's aesthetic preference for "odorlessness" that turns its normal secretion into a problem.
This guide consolidates 20 years of the most-misunderstood concepts from the consultation room into a single map — from anatomy through disease — of the apocrine gland. By the end you should be able to answer:
- How are apocrine, eccrine, and apoeccrine glands fundamentally different at the tissue level?
- Why are apocrine glands concentrated in the axillae, areolae, perineum, and ear canals?
- How does apocrine activity shift through puberty, reproductive years, and menopause?
- What's the full biochemical pathway from "odorless apocrine secretion" to "body odor"?
- Why does the ABCC11 genotype determine that 80–95% of East Asians have "dry earwax and no body odor"?
- What are the key differences in the apocrine disease spectrum — bromhidrosis, hidradenitis suppurativa, Fox-Fordyce disease, chromhidrosis?
- Which layer of the problem do "antimicrobial," "deodorant," and "antiperspirant" strategies actually address?
This isn't a treatment article — it's a medical-anatomy reference so you can see what's actually happening in your own body first. If you'd prefer to go straight to treatment options, jump to the Bromhidrosis Guide: Causes, Diagnosis, Treatment & Recovery or the Sweat Gland Surgery: Curettage vs Laser vs miraDry vs ETS.
Multi-site odor? If you have odor in more than one area, see the Odor Map for site-by-site triage first to identify the primary source before diving into this guide.
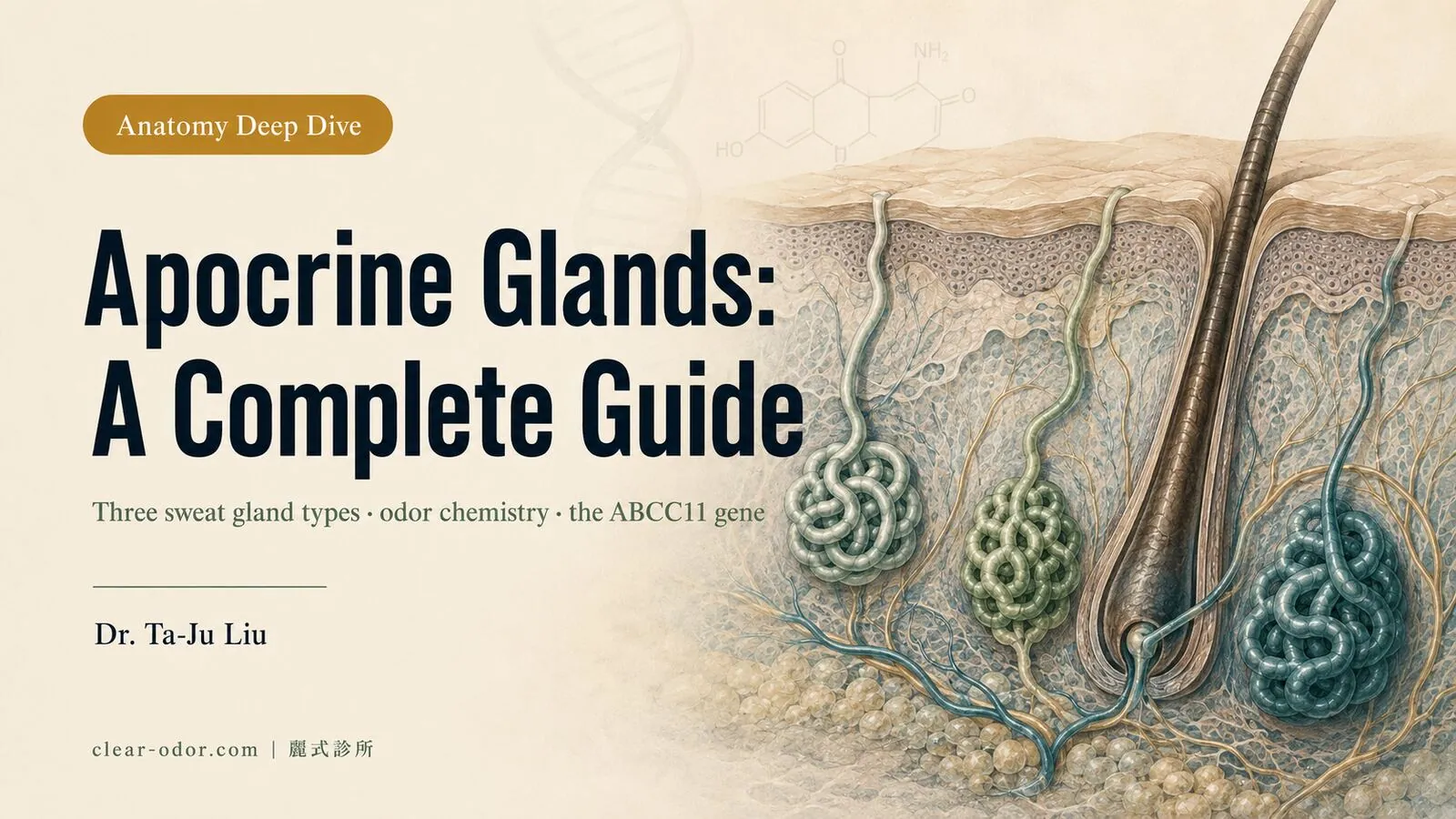
Apocrine, eccrine, apoeccrine — how do the three sweat glands differ?
The body actually has three sweat glands, not the usual two: apocrine glands are the source of body odor, eccrine glands produce the watery sweat that cools you, and apoeccrine glands are a high-output hybrid — telling these three apart is the first step to understanding every treatment.Most patient education says "the human body has two types of sweat glands." That's a simplification. The human body actually has three. Telling them apart is the first step toward understanding why treatments differ.
a. Eccrine Glands
- Count: roughly 2–4 million across the body, densest on the palms, soles, and forehead
- Distribution: present on virtually all skin, with the exceptions of the lips, external ear canal, and internal genitalia
- Structure: simple coiled tubular glands that open directly onto the skin surface
- Secretion: clear, hypotonic, 99% water, with small amounts of NaCl, urea, and lactate
- Function: thermoregulation — heat dissipation by evaporation, the core mechanism humans use to manage heat
- Odor: secretions are essentially odorless — body odor does not come from eccrine glands themselves
- Neural control: cholinergic sympathetic fibers (acetylcholine is the primary neurotransmitter)
Eccrine glands are functional from birth. Hyperhidrosis is a problem of this gland type — see the Hyperhidrosis Guide: Types, Severity, Treatments & ETS for details.
b. Apocrine Glands
- Count: roughly 2,000–4,000 across the body — 1,000 times fewer than eccrine glands
- Distribution: concentrated in the axillae, areolae, periumbilical area, perineum, external genitalia, peri-anal region, and external ear canal — this distribution isn't coincidence; it's the evolutionarily preserved pheromone-signaling zone
- Structure: larger, deeper, coiled tubular glands that open into the hair follicle, not the skin surface
- Secretion: milky, oily, containing protein, lipids, steroids, and fatty acid precursors
- Function: social and pheromone signaling (evolutionarily); in modern terms, mostly a marker of sexual maturity
- Odor: the secretion itself is essentially odorless — odor emerges only after the secretion interacts with skin microflora
- Neural control: adrenergic sympathetic fibers (norepinephrine), with significant hormonal modulation
c. Apoeccrine Glands
- Count: in adult axillae, roughly 10–45% of sweat glands, with substantial individual variation
- Distribution: axillae (some studies suggest small numbers may exist in the peri-areolar region)
- Structure: openings can be either at the skin surface or in the follicle — morphologically a hybrid of the other two types
- Secretion: clear, high-volume, similar to eccrine sweat but at a higher secretion rate
- Function: a major contributor to axillary "drenching sweat" — develops only after puberty
- Odor: largely odorless on its own, but the volume can dilute apocrine secretions while also creating a moist environment favorable for bacterial growth
Apoeccrine glands are a relatively recently characterized gland type (described by Sato and Sato in 1987) and remain a topic of ongoing research. Their existence explains why the axilla is both prone to heavy sweating and prone to odor — because all three sweat gland types are densely distributed in the same region.
Side-by-Side Comparison
| Dimension | Eccrine | Apocrine | Apoeccrine |
|---|---|---|---|
| Count | 2–4 million | 2,000–4,000 | 10–45% of axillary glands |
| Opening | Skin surface | Hair follicle | Skin or follicle |
| Secretion | Clear, hypotonic | Milky, oily | Clear, high volume |
| Primary function | Thermoregulation | Pheromone signaling | Axillary high-volume sweating |
| Native odor | Odorless | Odorless | Mostly odorless |
| Onset of function | Birth | Puberty | Puberty |
| Neural control | Cholinergic | Adrenergic | Mostly cholinergic |
| Related disease | Hyperhidrosis | Bromhidrosis, hidradenitis suppurativa, chromhidrosis | Amplifies hyperhidrosis |
Clinical viewpoint: Why do treatment strategies separate apocrine and eccrine glands? Because they're mechanistically different organs. Botox (blocking cholinergic signaling) works well on eccrine glands and only partially on apocrine glands. Surgical clearance of apocrine glands works for bromhidrosis and also for "pure hyperhidrosis" (because it simultaneously removes eccrine and apoeccrine glands). Treat bromhidrosis as if it were hyperhidrosis (or vice versa) and the outcome won't be good.
Where are apocrine glands located, and why concentrated in the underarms and areola?
Apocrine glands aren't evenly distributed — they concentrate in specific regions: underarms, areola, genital area, and ear canal. That's why odor in those areas is an apocrine issue (not an infection to suspect first), and why different sites need different treatment routes.Apocrine glands are not evenly distributed — they're concentrated in a few specific regions. Understanding this distribution serves two purposes: (1) it explains why "bromhidrosis at different body sites" requires different treatment paths; and (2) it explains why odor at certain sites is reliably an apocrine problem and doesn't need an infection workup.
Primary Distribution (High to Low Density)
| Region | Apocrine density | Clinical correlate |
|---|---|---|
| Axillae | Highest | Bromhidrosis, predilection site for hidradenitis suppurativa |
| Peri-areolar | High | Areolar odor; secretion around the Montgomery tubercles |
| Perineum, external genitalia, peri-anal | Medium-high | Perineal odor, perineal apocrine hyperplasia |
| External ear canal | Medium | Earwax type (this is the ABCC11-determined site) |
| Eyelids (glands of Moll) | Low | Glands at the eyelash root; related disease is rare |
| Periumbilical | Low | Occasional isolated odor |
| Nasal ala, nasal tip | Very low | Rare isolated cases |
Why This Distribution? An Evolutionary Lens
Apocrine glands cluster in hair-dense and skin-fold regions — which evolutionarily correspond to the optimal sites for pheromone release:
- Hair follicles provide a physical scaffold for secretion attachment and dispersion
- Skin folds create the temperature and humidity ideal for bacterial activity
- Even after we became upright walkers, these regions remained the "closest-perceptible" points to another person
In other words, our ancestors used these secretions to broadcast chemical signals about sexual maturity, health status, and emotional state. Modern society's odorless aesthetic has turned this evolutionary inheritance into a burden — but this doesn't make the apocrine gland itself "abnormal." It's a normal, functional organ that shouldn't be framed as a defect.
Treatment Differs by Site
- Axillae: highest apocrine density, finite surface area, fully surgically accessible — see the Axillary Bromhidrosis service page
- Areolae: apocrine glands interleave with mammary architecture; lactation function must be preserved — strategy differs from the axillae, see the Areolar Bromhidrosis service page
- Perineum / intimate regions: apocrine glands plus skin folds, microflora, and clothing-related heat retention interact in multiple ways — see the Perineal Odor service page
- External ear canal: earwax type is a phenotypic expression of ABCC11 genotype, not a disease — covered in detail in the next section
Clinical viewpoint: "I treated my axillary bromhidrosis and the areola or perineum still smells." This isn't a surgical failure — apocrine glands are independently distributed across body regions. Treating one site doesn't affect apocrine activity elsewhere. This needs to be understood before treatment planning, not after.
When do apocrine glands switch on, and how do they change with age?
Apocrine glands aren't functional from birth — they're switched on by hormones at puberty and shift again in midlife. That's one of their biggest differences from eccrine glands, and why body odor typically only becomes noticeable from puberty onward.The apocrine gland isn't functional from birth — this is one of its biggest differences from the eccrine gland.
Infancy to Childhood (Ages 0–10)
- Apocrine glands are histologically present, but secretorily inactive
- This is why children don't have body odor — not because the gland is missing, but because it hasn't been switched on
- Even with apocrine glands present, secretion is negligible and microflora has nothing to act on
Pubertal Activation (Ages 10–14)
- Sex hormones (androgens primarily, present in both sexes) rise sharply → apocrine glands are activated by hormonal stimulation
- Activation typically lags slightly behind other secondary sexual characteristics — body hair appears first, and apocrine secretion increases 6–12 months later
- Adolescent bromhidrosis is first noticed by the parent or the patient typically between ages 11 and 15
- This is why adolescent body odor is a normal developmental signal, not a disease — see the Kids' Body Odor: Normal Puberty or Clinical Bromhidrosis?
Reproductive Years (Ages 15–40)
- Apocrine activity is at the lifetime peak
- Significantly affected by menstrual cycle, pregnancy, lactation, stress, and diet
- Women may notice increased peri-areolar apocrine secretion during pregnancy and lactation (this is normal physiology)
- Men typically have stable and sustained high secretion during this period
Decline in Midlife (After Age 40)
- Estrogen decline after menopause in women → apocrine activity decreases noticeably — many women report "my body odor faded" after age 50
- Decline in men is slower and less uniform — androgens drop more gradually, and many men retain meaningful apocrine activity into their 60s
- This isn't being "cured" — it's physiological down-regulation of secretion; the glands themselves remain
Elderly Years (Age 70+)
- Apocrine activity approaches childhood levels
- Most older adults no longer have clinically significant bromhidrosis
- However, aging can introduce other body-odor sources — shifts in skin microflora, oxidation products of sebum (the so-called "old-person smell," 2-nonenal). These are unrelated to the apocrine gland and represent a different mechanism
What This Means for Treatment Timing
- Pre-puberty: surgery isn't indicated — the gland isn't active yet, so removal accomplishes nothing
- Ages 15–18 with confirmed moderate-to-severe bromhidrosis that affects daily life: surgery becomes reasonable — gland development has stabilized and outcomes are more predictable
- Around menopause: "natural attenuation" is a reasonable reason to defer surgery — but if daily life is already significantly affected, don't wait
- Operating too early has two risks: (1) gland development is incomplete and clearance may be inadequate; (2) residual glands may continue developing afterward
For detailed decision-making on pediatric surgical timing, see When Can Children Have Odor Surgery? A Parent's Guide.
How does an odorless secretion turn into body odor?
Apocrine secretion is itself odorless; it only becomes smelly after skin-surface bacteria break it down — a 4-step pathway from secretion to odor. That's exactly why the "antimicrobial" step can change the smell yet never cure it."Apocrine secretion itself is odorless" — patients often push back on this: "Then why do I smell?"
The key is that apocrine secretion is an odor precursor, not the odor itself. To become a perceptible body odor, secretion must pass through 4 steps.
Step 1: Apocrine Glands Secrete Odor Precursors
The milky, oily fluid secreted by the apocrine gland contains:
- Lipids: cholesterol, squalene, long-chain fatty acids
- Proteins: apocrine secretion-binding protein 1/2 (ASOB1/2) — these proteins are tightly linked to subsequent odor formation
- Steroids: DHEA-S, androsterone sulfate, 5α-androstenone, and other pheromone-like molecules
- Conjugated fatty acids: bound to protein and themselves odorless
When freshly secreted, these compounds are essentially imperceptible to human olfaction.
Step 2: Skin Microflora Cleave the Conjugates
The resident microflora of axillary skin primarily includes:
- Corynebacterium — the dominant producer of the most pungent bromhidrosis odor
- Staphylococcus — produces a more acidic, lighter odor
- Propionibacterium (now reclassified as Cutibacterium) — produces acidic compounds
- Anaerococcus — produces short-chain fatty acids associated with malodor
These bacteria (Corynebacterium especially) secrete enzymes (lipases, aminoacylases, and others) that cleave the protein–fatty acid conjugates in apocrine secretion, releasing free odor molecules.
Step 3: Free Odor Molecules Are Liberated
After enzymatic cleavage, the principal "bromhidrosis odor molecules" include:
- 3-methyl-2-hexenoic acid (3M2H) — the signature odor molecule of axillary bromhidrosis, carried and released by ASOB2 protein, and directly correlated in the literature with the "typical bromhidrosis smell"
- 3-hydroxy-3-methylhexanoic acid (HMHA) — a related short-chain fatty acid, odor-relevant
- 3-methyl-3-sulfanylhexan-1-ol (3M3SH) — an "onion-like" odor
- Androstenone, androstadienone — steroid derivatives. Some people are uniquely sensitive to these molecules due to polymorphisms of the olfactory receptor gene OR7D4
Step 4: Diffusion and Perception
Free odor molecules evaporate with body heat and mix with eccrine sweat, diffusing into the surrounding air. This is why exercise, stress, and heat intensify bromhidrosis: not because secretion volume changes, but because diffusion is amplified.
Mapping Treatments Onto the 4 Steps
| Strategy | Which step it targets | Limitations |
|---|---|---|
| Antiperspirants, powders | Reduces Step 4 diffusion environment | Doesn't eliminate the source; daily use required |
| Antimicrobial washes, antibacterial sprays | Reduces Step 2 microflora | Microflora rebounds; may disrupt the skin barrier |
| Laser hair removal | Reduces Step 1 follicle-associated microflora | Partial effect; doesn't remove apocrine glands |
| Botox | Reduces Step 1 secretion (via nerve blockade) | Wears off in 4–6 months |
| miraDry, laser sweat-gland ablation | Removes Step 1 glands | Blind delivery; clearance thoroughness is limited |
| Direct-visualization rotational curettage | Directly removes Step 1 glands | Requires an incision and 7 days of compression |
Clinical viewpoint: Why do we treat direct-visualization rotational curettage as our primary procedure? Because it reduces the supply at Step 1 — eliminate the upstream source and the downstream 3 steps lose their fuel. This is also why patients don't need daily antiperspirants or antimicrobials after surgery.
For comparison across treatment options, see the Sweat Gland Surgery: Curettage vs Laser vs miraDry vs ETS.
Why do 80–95% of East Asians have no body odor? It comes down to the ABCC11 gene
Body odor is largely decided by the ABCC11 gene: about 80–95% of East Asians carry the genotype that makes apocrine glands produce almost no odor, so they have no noticeable B.O. — proof that body odor is genetic constitution, not poor hygiene.If you've ever had genetic testing, you may have heard of ABCC11. It carries one of the most dramatic stories in apocrine biology.
What Is ABCC11?
- ABCC11 is a gene on chromosome 16q12.1
- It encodes an ATP-binding cassette transporter protein (a transmembrane transport protein)
- It's expressed in apocrine glands, ceruminous (ear canal) glands, and mammary glands
- Its function: transporting odor precursors (especially the conjugated form of 3M2H) into apocrine secretion
A Single SNP Rewrites the Secretion Profile
ABCC11 carries a key single-nucleotide polymorphism (SNP): rs17822931, a G→A point mutation at position 538.
- GG or GA genotype (dominant G allele): ABCC11 protein is expressed normally → apocrine glands secrete odor-precursor-containing milky, oily fluid → prone to bromhidrosis and wet earwax
- AA genotype (recessive A/A): ABCC11 protein is barely expressed → apocrine secretions lack odor precursors; ceruminous glands secrete dry earwax → minimal body odor and dry earwax
Striking Global Variation by Ancestry
| Population | A/A frequency (dry earwax + no body odor) |
|---|---|
| East Asian (China, Japan, Korea, Taiwan) | 80–95% |
| Southeast Asian | 30–50% |
| South Asian (Indian) | 30–50% |
| European | < 5% |
| African | < 5% |
| Indigenous American | ~30–50% |
This is why:
- Western culture treats deodorant as a daily essential — most of the population carries the G allele, with native apocrine secretion
- East Asians typically don't need antiperspirants — most are A/A and have minimal native body odor
- East Asians with bromhidrosis stand out more than Westerners do — because almost everyone around them is odorless, the few who aren't are conspicuous
- Earwax type is a useful self-screening clue — wet earwax usually maps to ABCC11 G genotype and potential apocrine odor-precursor secretion
But ABCC11 G ≠ Guaranteed Bromhidrosis
ABCC11 G is a necessary condition for bromhidrosis (A/A almost never produces it) — but it's not sufficient:
- Among G carriers, odor severity is modulated by other factors: apocrine density, skin microflora composition, other metabolic genes (FMO3 and others), and lifestyle
- Two G carriers can have very different odor intensity
- This is why Does Wet Earwax Mean Bromhidrosis? A Home Self-Check is "correlated but not absolute."
For the full inheritance pattern (dominant/recessive, parent-to-child expression), see Is Bromhidrosis Genetic? Inheritance & When to Check Kids.
Clinical viewpoint: I often use ABCC11 in clinic to correct a single misconception — bromhidrosis isn't a disease; it's genetics. It isn't an acquired hygiene problem, a dietary issue, or an endocrine abnormality. It's a normal genetic polymorphism, framed by modern society's odorless aesthetic as if it were a defect. Understanding this can reduce self-blame — and that emotional shift is an important step before any treatment begins.
Is bromhidrosis the only thing that goes wrong with apocrine glands?
No — beyond "normal secretion with strong odor" (bromhidrosis), apocrine glands can be the starting point of several genuine skin diseases; telling them apart keeps you from mistaking B.O. for a skin disease, or a skin disease for B.O.Beyond "normal secretion with strong odor" (i.e., bromhidrosis), several genuine diseases start at the apocrine gland. Distinguishing them prevents mislabeling "bromhidrosis" as "skin disease," or vice versa.
a. Bromhidrosis
- Nature: not a disease; one end of the spectrum of normal apocrine secretion interacting with skin microflora
- Features: a persistent or sweat-triggered characteristic odor in the axillae, areolae, perineum, or intimate regions
- Independent of sweat volume: bromhidrosis can occur with light sweating, and heavy sweating can be odorless
- Treatment: reduction of apocrine glands is the central principle
- See the Bromhidrosis Guide: Causes, Diagnosis, Treatment & Recovery
b. Hidradenitis Suppurativa (HS)
- Nature: a chronic inflammatory disease — this is a true disease, not a worse form of bromhidrosis
- Features: recurrent red nodules, abscesses, sinus tracts, and atrophic scars in the axillae, inframammary fold, intimate regions, and perineum
- Etiology: follicular occlusion plus sustained inflammation of the apocrine glands and superficial tissue, with bacterial infection, immune dysregulation, and familial predisposition as contributing factors
- Severity: Hurley stages I–III; stage III may require wide excision of involved skin
- Relationship to bromhidrosis: both cluster in apocrine-rich regions, but HS represents structural tissue destruction while bromhidrosis is functional odor only
- If HS is suspected: a formal dermatologic diagnosis is required; do not treat as bromhidrosis
- Risk of misdiagnosis: early HS treated as "recurrent axillary infection" with antibiotics — diagnostic delay can be years
c. Fox-Fordyce Disease (Apocrine Duct Hyperkeratosis)
- Nature: chronic skin disease caused by obstruction of the apocrine duct opening
- Features: dense, flesh-colored to pale-yellow, intensely itchy small papules in the axillae, areolae, or perineum, each centered on a hair follicle
- Epidemiology: predominantly affects women of reproductive age; uncommon in men
- Pathogenesis: apocrine secretion can't drain normally; duct rupture causes inflammation in surrounding tissue
- Relationship to bromhidrosis: usually has no distinctive odor — this is a "skin lesion" issue, not an "odor" issue
- Treatment: topical steroids, tretinoin, laser, and in rare cases surgical clearance
- Risk of misdiagnosis: years of unsuccessful treatment under the labels of "folliculitis" or "allergy"
d. Chromhidrosis
- Nature: apocrine secretions containing pigmented lipid compounds
- Features: yellow, green, blue, black, or red sweat in the axillae, areolae, or face — staining of clothing is the common chief complaint
- Epidemiology: extremely rare; one case might appear in years of practice
- Pathogenesis: accumulation of lipofuscin granules in apocrine cells; pigment is co-secreted
- Treatment: Botox can temporarily reduce secretion; topical ascorbic acid; severe cases may warrant apocrine clearance
- Relationship to bromhidrosis: chromhidrosis patients usually also have bromhidrosis (both reflect high apocrine activity)
e. Apocrine Carcinoma
- Nature: a rare malignant cutaneous neoplasm
- Features: a slowly enlarging nodule in the axilla, vulva, or peri-areolar region, often asymptomatic early
- Epidemiology: extremely rare, mostly in patients over 50
- Risk of misdiagnosis: early lesion mistaken for a sebaceous cyst or lipoma and watched
- If a persistent, larger-than-1-cm, irregularly shaped axillary mass is present, arrange a formal dermatology or general-surgery evaluation; don't assume "it's a bromhidrosis-related lump"
Quick Comparison: 5 Apocrine Conditions
| Disease | Primary presentation | Odor present? | Formal diagnosis needed? |
|---|---|---|---|
| Bromhidrosis | Persistent odor | Strong | No — it's a trait, not a disease |
| Hidradenitis suppurativa | Recurrent abscesses, nodules, sinus tracts | When infected | Yes — dermatology |
| Fox-Fordyce disease | Dense flesh-colored papules, intensely itchy | Usually none | Yes — dermatology |
| Chromhidrosis | Colored sweat staining clothing | Usually combined with bromhidrosis | Specialist evaluation |
| Apocrine carcinoma | Slowly enlarging firm nodule | Usually none | Yes — oncologic biopsy |
Clinical viewpoint: If your "underarm symptoms" come with firm lumps, recurrent abscesses, atrophic scars, dense papule clusters, or colored sweat — this is beyond simple bromhidrosis. A formal dermatology diagnosis first is safer than going straight to bromhidrosis surgery. When we see atypical presentations during the in-person consultation, we'll actively recommend a dermatology workup before discussing surgery.
Why can't "antimicrobial," "deodorant," or "antiperspirant" cure body odor?
Because all three work on the downstream of odor (bacteria, smell, sweat volume) — none touches the upstream apocrine gland itself. As long as the secretion source remains, the odor returns; that's why over-the-counter products can suppress but never cure.With the previous 6 sections as background, the opening question can finally be answered: "Why don't all these antiperspirant and deodorant products cure my body odor?"
Antimicrobials and Antibacterial Washes — Attack Step 2; Effect Disappears When Microflora Rebounds
- Antimicrobials reduce the resident skin microbiome
- But the microflora is a dynamic equilibrium — within 24–72 hours of stopping, density returns to baseline
- Excessive antimicrobial use disrupts the skin barrier and triggers compensatory overgrowth
- For ABCC11 G carriers (who produce odor precursors), the effect is only to "delay odor onset," not to eliminate it
Antiperspirants (Aluminum Salts) — Block Eccrine Glands, Bypass the Apocrine Gland
- The primary active ingredients (aluminum chloride, aluminium chlorohydrate) occlude the eccrine duct lumen
- Effective on eccrine glands (less sweat → less diffusion → less odor)
- But they have virtually no effect on apocrine glands — apocrine ducts open deep in the follicle, with different structure
- Effective for pure hyperhidrosis; only indirectly mitigates bromhidrosis
Deodorants and Perfumes — Mask Step 4 Diffusion
- Fragrance molecules cover the body's own odor
- They don't touch the source — the effect depends entirely on a diffusion race
- Heavy sweating breaks through the masking quickly
- Long-term use of certain fragrances can cause contact dermatitis in sensitive skin
Why Only Physical Removal Can Cure It
Back to the 4-step pathway: apocrine gland exists → secretes odor precursors → bacteria act → odor releases.
As long as Step 1 isn't addressed, any downstream intervention only "softens the symptom." Directly reducing the gland count at Step 1 is the shared core logic of surgery, laser, and miraDry. They differ only in how thoroughly and how precisely they reduce gland count.
See the Sweat Gland Surgery: Curettage vs Laser vs miraDry vs ETS and the Underarm Odor: Antiperspirant vs Botox vs Surgery for details.
So Are "Antimicrobials," "Deodorants," "Antiperspirants" Useless?
No. They have legitimate roles:
- Mild bromhidrosis (grade 1–2): antiperspirant plus good hygiene can maintain a socially undisturbed life
- Pre-operative bridge: temporarily reduce social burden while scheduling surgery
- Post-operative maintenance: in rare cases of residual mild odor, antiperspirant can manage day-to-day
- For patients unsuitable for or unwilling to undergo surgery: a tool for lifelong management, with the realistic expectation of daily use that can't be paused
The key is knowing exactly what strategy you're using and what level it achieves. Treating "daily antiperspirant" as a "cure" will frustrate you; treating "one-time surgery" as "never needing maintenance again" may also be over-optimistic (a small number of patients will have residual symptoms that still need managing).
Frequently Asked Questions
Q1: Do apocrine glands grow back after removal?
Almost never. Once apocrine glands have completed development at puberty, they don't regenerate the way skin or hair does. Residual glands after surgery can theoretically undergo compensatory hypertrophy under stimulation, but clinical recurrence after thorough direct-visualization rotational curettage is very uncommon (most studies report 5-year recurrence under 5%). What patients call "recurrence" is more often: (1) incomplete initial clearance; (2) major weight change altering residual gland distribution; or (3) untreated regions (areolae, perineum) continuing to secrete and being misperceived as axillary recurrence.Q2: Do apocrine glands have to be surgically removed? Can't medication suppress them?
There is currently no oral medication that can permanently shut off apocrine glands.
- Anticholinergics (glycopyrrolate and others) work on eccrine glands; effect on apocrine glands is limited
- Anti-androgens can theoretically reduce apocrine activity, but side effects are significant and not appropriate for body odor alone
- Botox temporarily reduces secretion, wears off in 4–6 months, with high long-term cost
- Topical inhibitors of ABCC11 are still experimental
So the "not surgery" option is long-term management (antiperspirant + hygiene + occasional Botox), not a cure.
Q3: Does pregnancy change apocrine activity in women?
Yes. Hormonal shifts during pregnancy can either intensify or reduce body odor — variation is significant. During lactation, secretion from peri-areolar apocrine glands and Montgomery glands both increase — this is normal physiology. We do not recommend peri-areolar apocrine surgery during lactation; wait until weaning and the mammary tissue stabilizes, then re-evaluate. Axillary surgery is technically possible outside lactation, but most surgeons (us included) recommend completing family planning before surgery to avoid pregnancy-related changes disrupting the result.Q4: Why do some patients still have "a faint smell" after surgery?
Apocrine surgery typically removes 80–95% of glands — not 100%. Reasons: (1) Safety: over-aggressive clearance damages dermal blood supply and sensory nerves, raising skin necrosis risk; (2) Anatomical variability: some glands sit deep, embedded in fat, and aren't fully reachable even under direct visualization; (3) Other regions (areolae, perineum) continue to secrete and aren't addressed by axillary surgery. Patients who want as close to "completely odorless" as possible can discuss a touch-up or supplementary miraDry — but understand that "100% odorless" isn't a biologically realistic expectation.
Q5: Are apocrine glands the same as sebaceous glands?
No. Sebaceous glands secrete sebum (oily, shea-butter-like) and also open into the follicle, but they're distributed across all hairy regions of the body (face and scalp predominantly) — completely different from the axillary, areolar, and intimate-region clustering of apocrine glands. Sebaceous-gland problems are acne, seborrheic dermatitis, and oily scalp. Apocrine-gland problems are bromhidrosis, hidradenitis suppurativa, and chromhidrosis. Scalp odor is primarily a sebaceous-microflora interaction, not an apocrine problem — see the Scalp Odor After Washing? The Microbiome & How to Manage.Q6: I'm still in puberty (ages 13–15) and noticed I have body odor. What should I do?
Don't rush to surgery. Reasons: (1) apocrine glands haven't completed development, so clearance may be incomplete; (2) puberty is still ongoing; surgery is better timed once secondary sexual characteristics have stabilized (regular menstrual cycles in girls, stable facial hair distribution in boys); (3) middle-school and high-school psychological stress can be managed with bridging strategies — antiperspirants, Botox, hygienic clothing choices. Surgery is generally deferred until around age 18. Very severe cases meaningfully affecting daily life may warrant an individualized decision with input from a pediatric medical team. See When Can Children Have Odor Surgery? A Parent's Guide.Q7: How much do male and female apocrine glands differ?
There are real differences: (1) men have slightly more glands on average and higher secretion volumes; (2) women have significant cyclical variation — luteal-phase secretion can exceed follicular-phase; (3) activity declines more slowly in men — women show clear decline after menopause; men can retain meaningful activity into their 60s–70s; (4) the odor composition differs slightly — androstenone derivatives are higher in men; 3M2H proportion is higher in women. The surgical principles are identical for both sexes, but planning differs — women need to consider family planning and lactation; men typically consider work-schedule timing.
Q8: Can apocrine secretion be "detected" via sweat testing?
Most sweat-based testing (occupational toxin metabolite testing, athlete doping panels) targets eccrine secretion, which differs from apocrine secretion. Apocrine secretion is low-volume and not easily captured in standard sweat samples — apocrine research relies on skin swabs or axillary absorbent pads. Standard daily sweat testing doesn't directly reflect apocrine activity.
Q9: Does apocrine surgery affect sweating?
Yes — and that's part of the therapeutic effect. Direct-visualization rotational curettage simultaneously removes apocrine, eccrine, and apoeccrine glands — axillary sweating noticeably decreases post-op (60–80% in most patients), which is a double benefit for combined bromhidrosis + hyperhidrosis patients. The body still sweats normally from other regions (palms, soles, trunk, scalp) — thermoregulation isn't impaired. A small minority feel "I sweat more elsewhere" after surgery — this is local regulatory rebalancing, fundamentally different from the true compensatory hyperhidrosis after ETS. The latter is an irreversible result of nerve transection; the former is the relative perception of local gland reduction.Q10: Do apocrine glands respond to emotion and stress?
Yes, strongly. Apocrine glands are controlled by adrenergic nerves — stress, anxiety, excitement, and sexual arousal all cause a sudden surge in apocrine secretion. This is why odor often intensifies under stress. Evolutionarily, this is part of emotional chemical signaling. In clinic, anxiety-prone patients often perceive odor fluctuating with emotion — surgery alone may not fully resolve the perception. Psychological intervention for anxiety (CBT, relaxation training) is sometimes as important as the surgery itself.Q11: Does diet really affect apocrine odor?
It affects it, but it's not the primary driver. Specific foods (garlic, onion, curry, cumin, red meat) can temporarily shift axillary odor composition, but they don't increase apocrine gland count or long-term activity. Short-term dietary changes can soften the smell a bit, but they can't cure the underlying tendency. See Does Diet Affect Body Odor? Garlic, Red Meat & Alcohol.Q12: Can hidradenitis suppurativa (HS) patients undergo bromhidrosis surgery?
Not as a simple bromhidrosis procedure. HS is a chronic inflammatory disease — surgery must center on controlling HS as the goal. This typically requires: (1) formal dermatology assessment of severity (Hurley I–III); (2) inflammation control (antibiotics, biologics); (3) for severe cases, wide excision of all affected skin by a dermatologic or plastic surgeon — a fundamentally different operation from "bromhidrosis surgery." If you have recurrent axillary abscesses, sinus tracts, or atrophic scars, see a dermatologist for diagnosis first. Don't treat it as "worsening bromhidrosis."Related Reading
- Bromhidrosis Guide: Causes, Diagnosis, Treatment & Recovery
- Sweat Gland Surgery: Curettage vs Laser vs miraDry vs ETS
- Is Bromhidrosis Genetic? Inheritance & When to Check Kids
- Aging Body Odor vs Bromhidrosis: 3 Smells, How to Tell
- Stale Smell on Your Pillow After 40? 2-Nonenal Explained
- Body Odor, Sweat Smell & Bromhidrosis: 3 Different Smells
- Axillary Bromhidrosis
- Areola Bromhidrosis
- Perineal Bromhidrosis
- Pediatric Bromhidrosis
- Midlife Body Odor & Aging Odor Guide
Conclusion: Treat the Apocrine Gland as a Normal Organ, Not the Enemy
The apocrine gland is not a defect, not a disease, not an abnormality — it's a normal pheromone organ preserved by human evolution. Its secretion can be a social burden under modern aesthetics, but that's a problem of social context, not of the individual's biology being "wrong."
Understanding this allows a calmer treatment decision:
- For people with mild odor that doesn't affect daily life: acceptance and management is a reasonable choice — antiperspirants, hygiene, and clothing selection are enough
- For people with moderate-to-severe odor affecting social life, work, or mental health: gland reduction surgery is letting a normal organ operate within a range you choose — not "eliminating an abnormality"
- For patients with the genuine disease spectrum (HS, Fox-Fordyce, chromhidrosis): secure a formal diagnosis first — the treatment path differs entirely from straightforward bromhidrosis
If you'd like Dr. Liu to personally palpate apocrine distribution, review family history, and discuss the treatment pathway best suited to your situation, request a consultation. Dr. Ta-Ju Liu has 20 years of focused experience in odor and sweat surgery and over 10,000 cases — and can help you understand the apocrine physiology of your own body before deciding on any strategy.
This article is for educational purposes; individual outcomes vary. Actual treatment and suitability require an in-person evaluation by Dr. Ta-Ju Liu. The anatomical, physiological, and genetic data cited here are based on currently published medical literature, and future research may update some details. Hidradenitis suppurativa, Fox-Fordyce disease, chromhidrosis, and apocrine carcinoma require formal diagnosis by a dermatologic specialist; this article does not constitute individualized diagnosis or treatment advice.